A Race Against Heat and Time: A Severely Ill Elephant, A Team That Chose Precision Over Noise
Some rescues begin as a rumor in the dust—signs soft enough to miss, strong enough to matter.
In a dry corridor of savanna where wind scribbles over old tracks, rangers noticed something wrong long before anyone reached for a radio.
An adult elephant cow lingered at a waterhole, drank slow, and stood with her head low and ears half-opened in the posture that says breath is expensive.
She drooled thick saliva, swayed slightly to keep balance, and lifted a forefoot only to let it down again without conviction.
The herd stood like punctuation around her—matriarch at a respectful distance, adolescents trying on bravery, calves pressed against their mothers to learn by quiet observation.
The cow’s eyes told the real story: tired, aware, not defeated.

What followed did not turn a wild giant into a hospital patient.
It widened the margin so she could keep her life where it belongs.
The moment that melted hearts happened in plain quiet daylight, when the team’s restraint allowed dignity to stay put.
Below is a structured account—how the problem was read, why the plan favored field medicine over control, and how doing exactly enough became the bravest choice in a landscape that punishes hurry.
The Place: Heat, Dust, and the Rules of Distance
Picture a shallow basin where mud at the water’s edge remembers last week’s rain but the rest of the valley has forgotten.
Acacia shade moves across the ground in small increments, teaching patience to those who need it.
Tracks compete for space—antelope in quick commas, warthog carving short exclamations, elephants laying down long sentences with confidence and weight.
The affected elephant held herself apart but not alone, facing a line of scrub that cut wind to a tolerable thread.
Her trunk hung with effort, lifted occasionally to test air and scent.
She was thin for a matriarchal herd’s standards—hipbones sharper than usual, temporal depressions deepened, ribs writing faint lines under hide.
Flanks rose and fell in shallow cycles that meant work.
No obvious wounds.
No snare.
Illness, not trap.
Rangers kept distance, counted breaths from binocular shadows, and radioed without drama: adult elephant female, depressed posture, labored breathing, drooling, reduced appetite, herd present and calm, risk of dehydration and systemic illness.
The call went out with the tone that respects complexity.
First Reading: Facts Before Feelings
The field veterinarian—Dr.
Meera—arrived with a compact kit and a way of moving that sets matriarchs at ease.
She approached downwind, in arcs, kneeling at intervals, hands visible.
She let the herd read her before she read the cow.
- Posture: head low, ears semi-open, trunk relaxed with intermittent lift; occasional sway to ease muscle fatigue.
- Respiration: elevated and shallow; intermittent soft cough; nasal discharge minimal.
- Hydration: borderline to low; long, slow drinking with pauses; thick saliva; depleted skin turgor.
- Temperature: likely elevated (confirmed later); heat stress compounding breath effort.
- Behavior: alert but fatigued; not aggressive; attention divided between herd and own body.
- Herd dynamics: matriarch watchful, adolescents posturing on the edges, mothers keeping calves in educational proximity; no charging.
Differentials: respiratory infection (bacterial or viral), heat stress with secondary dehydration, early colic with gas distension, parasitic burden elevating systemic strain, oral lesion or dental pain exacerbating drooling, toxin exposure (less likely given herd condition), or a combination of infection and heat.
The absence of obvious trauma focused the plan on internal medicine.
Decision: treat in place.
Use minimal, reversible sedation only if necessary for procedures.
Prioritize aggressive hydration, antipyretics, targeted antibiotics if infection suspected, anti-inflammatory support sized to elephant physiology, and careful monitoring.
Avoid transport unless collapse or diagnostic necessity demands it.
Keep the herd’s geometry intact.
The Plan: A Ladder of Small, Correct Choices
The plan read like a quiet checklist that refuses performance:
- Approach: downwind arcs; no direct lines; vehicles positioned as gentle barriers only if adolescents test boundaries.
- Sedation: avoid full sedation if possible; consider low-dose tranquilization for IV placement if necessary; reversal agents ready; oxygen staged.
- Diagnostics: handheld ultrasound for thoracic and abdominal screening; thermal imaging for surface heat mapping; blood sampling via ear vein catheter for CBC and chemistry; visual oral exam if tolerated.
- Support: warmed isotonic fluids delivered via gravity-fed ear vein line; antipyretic dose calibrated to body mass; broad-spectrum antibiotic if clinical signs support infection; anti-inflammatory sized to comfort without kidney insult.
- Environmental: shade screen angled to cut harsh light; portable fan directed at ground-level to move air without spooking; water access maintained; mud wallow encouraged for thermoregulation.
- Herd management: one ranger reading matriarch; one following adolescents; quiet voices; radios trading numbers and times; no horns, no shouting.
- Recovery and monitoring: step back early; observe at distance for two hours; reassess at dusk and dawn via camera traps; escalate only if deterioration overtakes.
Restraint is not inaction.
It is ambition tuned to reality.
The Approach: Asking Permission the Elephant Way
Permission in elephant grammar comes as a refusal to escalate.
The matriarch’s ears softened after a minute.
The affected cow lowered her trunk, then lifted it toward Dr.
Meera, reading scent and intent.
A shade screen slid into place at a respectful distance; the fan laid a low drift of air across ground-level heat.
The herd watched, then rebalanced into a relaxed geometry that turned drama into routine.
IV access was the first challenge—ear veins can be generous and stubborn.
Dr.
Meera worked with slow hands, gentle traction, and a fine-gauge catheter sized for pachyderm tissue.
A microdose of tranquilizer softened resistance without stealing breath.
The catheter slid in and held.
Warm fluids began to move.
Hydration is not a single act; it is a quiet conversation between vein, heart, and need.
The cow’s eyelids softened by degrees.
Ears spread farther open—an elephant’s sign that air and heat are under negotiation.
Diagnostics in the Field: Enough Information, No Theater
Handheld ultrasound mapped lungs with a limited but useful view: mild B-lines suggestive of interstitial changes—consistent with respiratory infection or inflammation; no large pleural effusion.
Abdominal scan showed gas pockets without severe distension; gut motility present, not ideal.
Thermal imaging painted hotter regions along forehead and flank—consistent with fever and heat stress.
Blood sampling told truths that would be confirmed later in a lab: elevated white cell count suggesting infection, mild electrolyte imbalance, signs of dehydration.
No red flags screaming catastrophe; a chorus warning diligence.
An oral check showed mild gum inflammation, slight ulceration at the tongue edge—irritating but not the main story.
Drooling likely a combination of fever, dehydration, and oral discomfort.
Clinical picture: respiratory infection layered with heat stress and dehydration, minor oral lesions contributing to salivation, gut motility slowed but present.
Treatment That Doesn’t Announce Itself
- Hydration: warmed isotonic fluids in staged volumes, avoiding overload; small bolus followed by steady drip; watch heart rate and respiration for response.
- Antipyretic: dose calibrated to elephant mass; fever downshifts reduce respiratory load and improve comfort.
- Antibiotics: broad-spectrum administration IV and IM—swift onset, durable cover; choice tuned to likely pathogens in savanna conditions.
- Anti-inflammatory: conservative dose for pain and systemic relief, protecting renal function in heat.
- Electrolytes: supplemental correction to support cardiac and muscular function.
- Comfort measures: shade and airflow maintained; mud access encouraged; water placed to minimize walking cost.
The cow’s breath deepened as fluids climbed into circulation.
Ears cooled.
Trunk lifted with more curiosity than obligation.
The matriarch eased closer—no threat, just presence.
Adolescents performed one last half-hearted bluff and gave up, bored by competence.
The Heart-Melting Moment: A Trunk on a Shoulder, A Treaty Kept
It wasn’t the IV line that melted hearts.
It was what happened after.
As the antipyretic settled and the fluids did their quiet work, the cow extended her trunk and laid it lightly across Dr.
Meera’s forearm—no pressure, no panic, just contact.
It lasted a breath, then another.
Then she withdrew and turned her head toward the herd.
The gesture read as thanks to human eyes and as acknowledgment to those who work in this language daily: a treaty honored.
Help arrived as a guest and stayed long enough to matter.
The clip traveled later—a few seconds of quiet touch, a camera kept at distance, no staged angle.
The moment went viral because it felt like permission caught on film.
Recovery Through the Afternoon: Small Wins Stacked
Two hours later, her respiratory cadence slowed.
Drooling decreased.
She drank longer without stopping and created a shallow mud wallow with her forefoot—a self-prescribed cool-down that capped the team’s efforts.
The herd moved to shade.
The cow remained upright, rested with trunk coiled lightly, ears set to half-sails that read comfort rather than distress.
The IV line came out clean.
The catheter site was dressed with scent-neutral barrier film.
Rangers reset vehicle angles to reduce visual pressure and let the place become a place again.
Dusk brought cooler air.
The cow walked twenty yards toward thicker shade, paused, and defecated—normal consistency, a relief and a data point.
She stood easier.
The matriarch brushed her flank with trunk-tip and held steady as night took the valley.
Forty-Eight Hours: Proof in Ordinary Behavior
Camera traps recorded the morning in spare frames that carried weight:
- Dawn: longer drink, square stance, trunk active with exploratory arcs; drooling minimal.
- Midday: mud wallow repeated; ears open and cool; standing rest more frequent, lying rest returning in short intervals—confidence to recline means trust in breath.
- Evening: browsing resumed; small leaves and pods chosen for ease; gut motility improved.
Lab confirmations lagged behind behavior but matched the field’s calculus: infection trending down with antibiotics onboard, electrolytes stabilizing, hydration improved, mild anemia from stress correcting naturally.
No staged updates.
No hovering.
The herd carried the rest of the story forward.
Day Three to Day Ten: Strength Returning in Quiet Lines
- Day three: respiratory rate near baseline; cough rare; drooling resolved; appetite increased; drinking regular.
- Day five: longer walks with herd; adolescent antics ignored with queenly efficiency; mud baths turned from necessity to comfort.
- Day seven: noticeable weight on the return path to water; gait fluid; trunk play with a calf—small taps, short lifts, patience in teaching.
- Day ten: behavior fully ordinary—feeding, moving, resting as a unit; matriarch’s geometry relaxed; adolescents bored again, which is a perfect outcome.
Field notes read like understatement: “Breath easy.
Appetite strong.
Cohesion intact.”
Why This Worked: Principles Hidden in Restraint
- Treat in place preserved social bonds and reduced stress.
Hospitals offer machines; herds offer maps and safety the machines can’t replicate.
- Minimal sedation protected breathing and orientation.
Calm without collapse allowed procedures with fast recoveries.
- Targeted medicine beat theatrics.
Hydration, antipyretics, antibiotics, and electrolytes—small correct interventions saved more than big gestures would.
- Environmental tweaks by inches mattered.
Shade, airflow, and mud access reduced physiological load without turning wild ground into a ward.
- Exit discipline completed care.
Leaving early prevented help from becoming custody.
Precision did the heavy lifting; humility kept it honest.
The Human Craft: Tools, Training, Boundaries
Under the calm operation lived a scaffold of practiced choices:
- Field-ready gear: fine-gauge ear-vein catheters; gravity-fed fluid rigs; handheld ultrasound and thermal imaging; pulse oximetry suited to thick lips; scent-neutral barrier films.
- Pharmacology tuned to pachyderms: weight-calibrated antipyretics, antibiotics with appropriate spectrum and half-life, anti-inflammatories sized to protect kidneys in heat.
- Communication discipline: radios trading numbers, times, and dosages—not adjectives; one lead voice; contingency plans spoken once and understood.
- Boundary respect: no collars unless medically necessary; no branding; no staged photos; no turning a private struggle into content.
The team moved like guests.
The herd answered like hosts who approve of company that knows when to leave.
The Moment That Melted Hearts, Revisited
The clip of the trunk resting lightly on a human arm held the world’s attention because it showed restraint from both sides.
The elephant did not demand, and the humans did not claim.
It was a conversation in touch, not a contract in control.
People called it gratitude; professionals called it communication.
Either way, it translated into trust.
The second, quieter clip mattered as much: the cow stepping into a mud wallow and lowering herself with care, breath steady, eyes soft—the camera staying back, the team already gone.
Recovery belongs to the animal, not the audience.
A Month Later: The Update That Matters More Than Headlines
- Week two: no fever spikes; respiratory rate steady; appetite robust; hydration normal; oral ulcers resolved.
- Week three: herd ranged farther; waterhole visits efficient; adolescent antics resumed without consequence; calves shadow-played trunk taps like apprentices.
- Week four: no relapse; lab follow-up via dung and saliva sampling from ground checks indicated low parasite burden and no active infection markers; routine patrols resumed; camera traps reduced to baseline fronts.
The rescue exited the animals’ story as cleanly as a foot lifts from damp sand.
The valley kept time with wind.
Lessons That Travel
- Function first.
In wild medicine, the fastest path to survival is restoring breath, hydration, and comfort so the animal can participate in its own recovery.
- Autonomy is health.
If help erases social bonds or orientation, the gain may be an illusion and the cost too high.
- Field medicine can be enough.
Hydration, fever control, targeted antibiotics, and quiet perimeters often outperform clinical transport for wild patients.
- Time heals when pressure is low.
Lower the load, keep resources near, and let biology finish the chapters humans shouldn’t write.
- Dignity is a metric.
If the animal leaves more itself than when help arrived, the plan was sized right.
These rules fit in a kit and in a mindset—and they travel well.
What Endures: Images Strong Enough to Stay
Strip away logistics and keep the scenes that refuse to fade:
- A large shadow under acacia, ears half-opened, trunk testing air while breath finds steadier ground.
- Warm fluids moving into a vein, not as a spectacle, but as a promise made with discipline.
- A trunk resting lightly on a human forearm—contact sized to trust, not drama.
- A mud wallow accepting weight as breath turns from cost to capacity.
- A herd resuming its map—matriarch anchoring, adolescents practicing theater, calves learning the grammar of survival.
Some rescues need sirens and floodlights.
This one needed shade, water, skill, and restraint.
Somewhere on that savanna, under a sky that writes long stories in heat and rain, an elephant breathes easy again, moves with the confident economy her size deserves, and leans into companionship shaped by memory and sound.
And a small team drives away along a dusty track with a steady conviction: the best missions aren’t about proving what we can do—they’re about knowing exactly when to help, precisely how gently to do it, and when to leave so life can belong to itself again.
News

A Single Dad Helped a Deaf Woman at the Airport — He Had No Idea Her Daughter Was a CEO!..
I was standing in the middle of one of the busiest airports in the country, surrounded by hundreds of people rushing to their gates, dragging suitcases, staring at their phones, completely absorbed in their own little worlds. And in the middle of all that chaos, there was this older woman, elegantly dressed, silver hair pinned […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked
They were told they would be stripped, punished, paraded. Instead, they were told to line up and handed dresses. The boots of the guards thudded softly against dry Texas soil as the sun climbed higher. A line of exhausted Japanese women stood barefoot in the dust, their eyes hollow, their uniforms torn. They had once […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 2
Another girl flinched when a medic approached her with a stethoscope. She covered her chest with both arms. Trembling, the medic froze, then slowly knelt down and placed the stethoscope against his own heart, tapping it twice, and smiled. She didn’t smile back, but she let him listen. One girl had a bruised wrist, deep […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 3
The field where they had learned to laugh again, the post where someone always left tea, the porch where banjos had played. And the men, the cowboys, the medics, the guards, they stood watching, hats in hand. Not victors, not jailers, just men changed, too. Because the truth was the war had ended long ago. […]
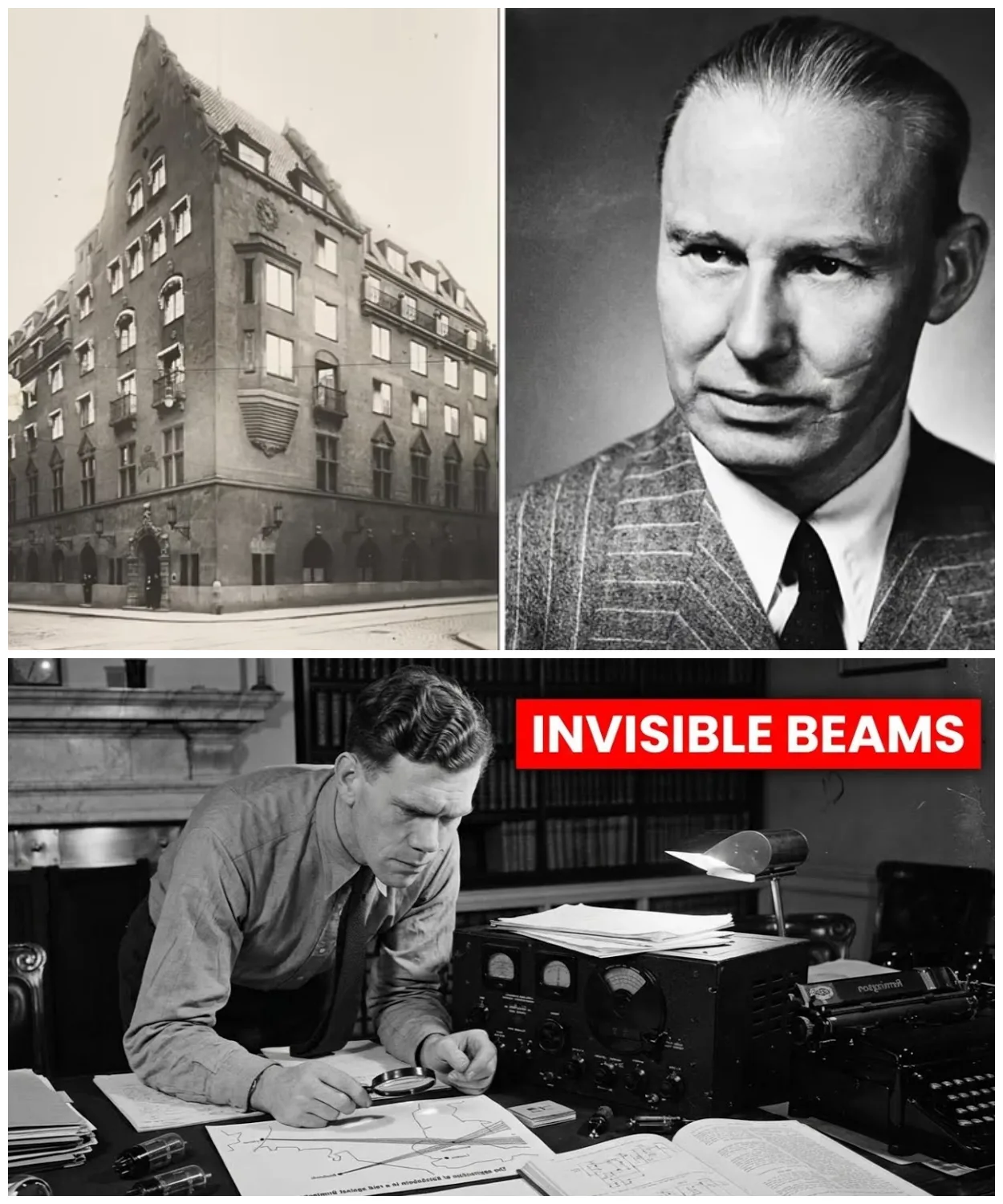
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio
June 21st, 1940. 10 Downing Street, the cabinet room. Reginald Victor Jones arrives 30 minutes late to a meeting already in progress. He’s 28 years old, the youngest person in the room by decades. Winston Churchill sits at the head of the table, 65, prime minister for 6 weeks. Around him, Air Chief Marshall Hugh […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio – Part 2
She memorizes them near photographic memory. Her September 1943 WTEL report identifies Colonel Max Waktell, gives precise operational details, maps planned launch locations from Britney to the Netherlands. When Jones inquires about the source, he’s told only one of the most remarkable young women of her generation. Rouso is arrested in April 1944. Survives three […]
End of content
No more pages to load