From a quiet Brentwood street, the house looked ordinary—well‑kept lawn, soft lamps in the windows, the kind of calm that suggests a life running on schedule.
Inside, the schedule had been replaced by custody time.
A life that once moved by rehearsals and dinners now moved by pill calls, welfare checks, and the click of a steel door that never forgets to close.
That is the geography Nick Reiner woke up to after his arrest: not prison but a county jail built as a bridge between the courts and the hospitals, known in Los Angeles as Twin Towers Correctional Facility.
In public conversation, people talk about survival as if it were a verdict.

In reality, survival here is a sequence of small acts—sleep, medication, routine—and the luck of being classified where the danger is lower than the night.
Twin Towers is not a cinematic villain.
It is a complicated institution inside a complicated system: a medical‑mental health jail that houses detainees who are awaiting trial or serving short county terms, many flagged for psychiatric supervision.
It cannot be understood as a single hallway with a single story.
On paper, the place provides evaluations, crisis stabilization, medication management, and access to county hospital services when needed.
In practice, it bears all the weaknesses large urban jails know too well—overcrowding at times, maintenance that lags, hygiene that ebbs and flows with budgets and staffing, and a built environment of concrete and steel that treats sleep like a rumor.
For someone who has lived most of life buffered by family resources, the transition is less a fall than a change in atmosphere: the lights stay on, the air is thin, and every sound travels.
A high‑profile detainee is classified by more than a last name.
Charges, documented mental‑health history, custody behavior, and vulnerability to assault all feed into housing decisions.
The system has levers for protection—psychiatric modules, special needs yards, separated movement—but nothing inside a jail is absolute.
Risk can be lowered; it cannot be erased.
The stories that travel fastest are the ones about shouting at night, about talking to a wall, about the quiet a person keeps when nothing in the room is quiet.
Some of those stories are true, some stretched, some misplaced.
What matters for the court is what gets written down: nursing notes, incident reports, psychiatric evaluations, observations in hearings.
A safety garment, for example—the shapeless smock with no strings—is a signal of custody concern, not a diagnosis.
It says staff fear self‑harm, not that staff know anything with certainty about the future.
To understand what could happen next, it helps to separate two ideas the public often blurs.
Competency asks whether the defendant, at the time of proceedings, understands the nature of the charges and can assist counsel.
If not, the court pauses the case and orders treatment, often at a state hospital, until competence is restored.
Insanity is a different question entirely: whether, at the time of the alleged offense, a mental disease or defect kept the defendant from understanding the nature and quality of the act, or from knowing it was wrong.
In California, that is a narrow standard.
Medication changes weeks before an incident, long records of diagnosis, evidence of substance use—all may be relevant to one or both questions, but none decide the outcome alone.
Judges and juries listen to experts, read records, and weigh behavior around the alleged act.
If a jury finds a defendant not guilty by reason of insanity, the door does not open onto freedom.
It opens onto a locked hospital where confinement is measured not by a calendar sentence but by clinical risk.
For violent charges, decades are common.
Progress is a ladder of treatment, privileges, and supervised steps back into the world, if ever.
If, instead, a defendant is convicted of two counts of first‑degree murder, the door opens onto the state prison system: movement becomes tighter, yards may be sensitive‑needs rather than general population, mental‑health care is delivered within a different set of rules, and time is counted by program slots and parole rules—sometimes without parole at all.
Inside any carceral space, the most durable danger for someone with psychiatric fragility is internal.
Fluorescent nights, disrupted sleep, irregular routines, and the stress of confinement can erode attention, memory, and will.
Medication helps; inconsistent delivery hurts.
Therapy exists; logistics make it hard.
Staff can be vigilant; populations churn and stretch capacity.
When people outside say “he won’t survive prison,” they often mean “we fear what happens when a fragile mind meets an unforgiving institution.” That fear is not foolish.
It’s just not prophecy.
Protective housing and psychiatric units reduce exposure to the kinds of violence people imagine; isolation and the grind of routine introduce different harms that are slower and less visible.
It is tempting, given the history of privilege around a famous family, to write a neat narrative: a life cushioned by money, then a life stripped by steel.
The cushion was real.
The steel is, too.
But inside the medical floors of a county jail, the currency is clinical.
A nurse does not care who paid for a rehab a decade ago.
A clinician cares whether the current medication is titrated correctly, whether the person is eating, whether the stare is far away for too long, whether words line up in a way that suggests dangerous drift.
A deputy cares whether the module is calm and whether a person follows orders without triggering a cascade.
In that way, institutions can be both indifferent to the past and attentive to the present.
The rumors that describe a detainee spiraling—hoarse denials repeated like a scratched record, a hand pounding steel without clear purpose, a voice shifting between adult and child, phrases addressed to someone who isn’t in the room—are the vocabulary of custody life.
Sometimes they mark psychosis.
Sometimes they mark panic’s choreography.
Sometimes they are the composite of several people overlaid onto one.
The defense will do what defenses do when faced with severe charges and mental‑health history: contest competency if warranted, consider an insanity plea if evidence supports it, and file conditions‑of‑confinement motions when they believe custody is harming their client beyond constitutional tolerances.
The prosecution will counter with its own experts and narratives.
The court will decide, slowly and with paperwork.
The question people ask most—what will happen to him—has honest answers that sound thin because they respect uncertainty.
If he remains in county custody pretrial, expect cycles of observation, medication rounds, and hearings.
If he is found incompetent, expect hospital treatment to restore competence, then a return to court.
If he is found sane and guilty, expect state prison with mental‑health services and a classification that errs on caution.
If he is found NGRI, expect a locked hospital with an indeterminate horizon measured by risk, not by calendar.
In every branch, the system keeps two obligations at once: to hold a person accountable where proof warrants it, and to treat illness where medicine demands it.
It does not always do both well.
It is built to try.
There is a different question worth asking because it matters regardless of any verdict: what does safety look like for the surviving family, and for the public watching systems they fund? Safety inside custody is classification and observation that work.
Safety outside custody is avoiding the seductive cruelty of writing anyone’s fate as a headline and calling the work done.
The work is audits of staffing, budgets for clinicians, fixed rounds done on time, grievance systems that function, and courts that check on what they order rather than assuming it happened because ink dried.
For people who want a sharper picture of how this story might unfold without claiming knowledge no one has, a few realities are steady.
Jail is not prison; it is a holding environment with medical floors and churn.
Competence is about now; insanity is about then.
Protective housing exists; it reduces certain risks and heightens others.
State hospitals are not escapes; they are long confinements organized around clinical criteria.
Prisons have mental‑health programs that can be humane or thin, depending on the facility and the person’s classification.
None of these environments are designed for hope.
People inside them make hope anyway, sometimes with routine, sometimes with a book, sometimes with a pill that smooths an edge without erasing it.
The story you began with—“won’t survive prison”—is a cry, not a fact.
It carries the grief and fury of what has been alleged, and the panic any human feels when imagining a fragile person in a hard place.
It is not how policy should be written.
Policy is written by counting what has happened in similar cases and building processes that lower risk, not in predicting the end of one life to satisfy the human desire for closure.
Closure, in cases like this, rarely arrives.
Courts deliver outcomes.
Families try to live after them.
Outside the walls, people who loved Rob Reiner’s work and Michelle’s presence will keep telling their stories about kindness learned from art and attention learned from a person who saw them clearly.
Inside, the person at the center of the case will keep living a smaller life: a rack, a tray, a light that does not go off, a routine pressed onto a nervous system that was never good at routines.
That is not an argument for mercy over accountability, nor for punishment over care.
It is the truthful texture of custody life for a mind under stress.
If there is a single sentence that does more good than any prophecy, it is the small one that governs institutions when they work: watch closely.
Watch the rounds and the meds and the rooms and the records.
Watch the court dates and the transfers.
Watch the edges of a person’s mind for fray and the edges of a system for failure.
Watching is not enough.
It is where the next right act begins.
News

A Single Dad Helped a Deaf Woman at the Airport — He Had No Idea Her Daughter Was a CEO!..
I was standing in the middle of one of the busiest airports in the country, surrounded by hundreds of people rushing to their gates, dragging suitcases, staring at their phones, completely absorbed in their own little worlds. And in the middle of all that chaos, there was this older woman, elegantly dressed, silver hair pinned […]
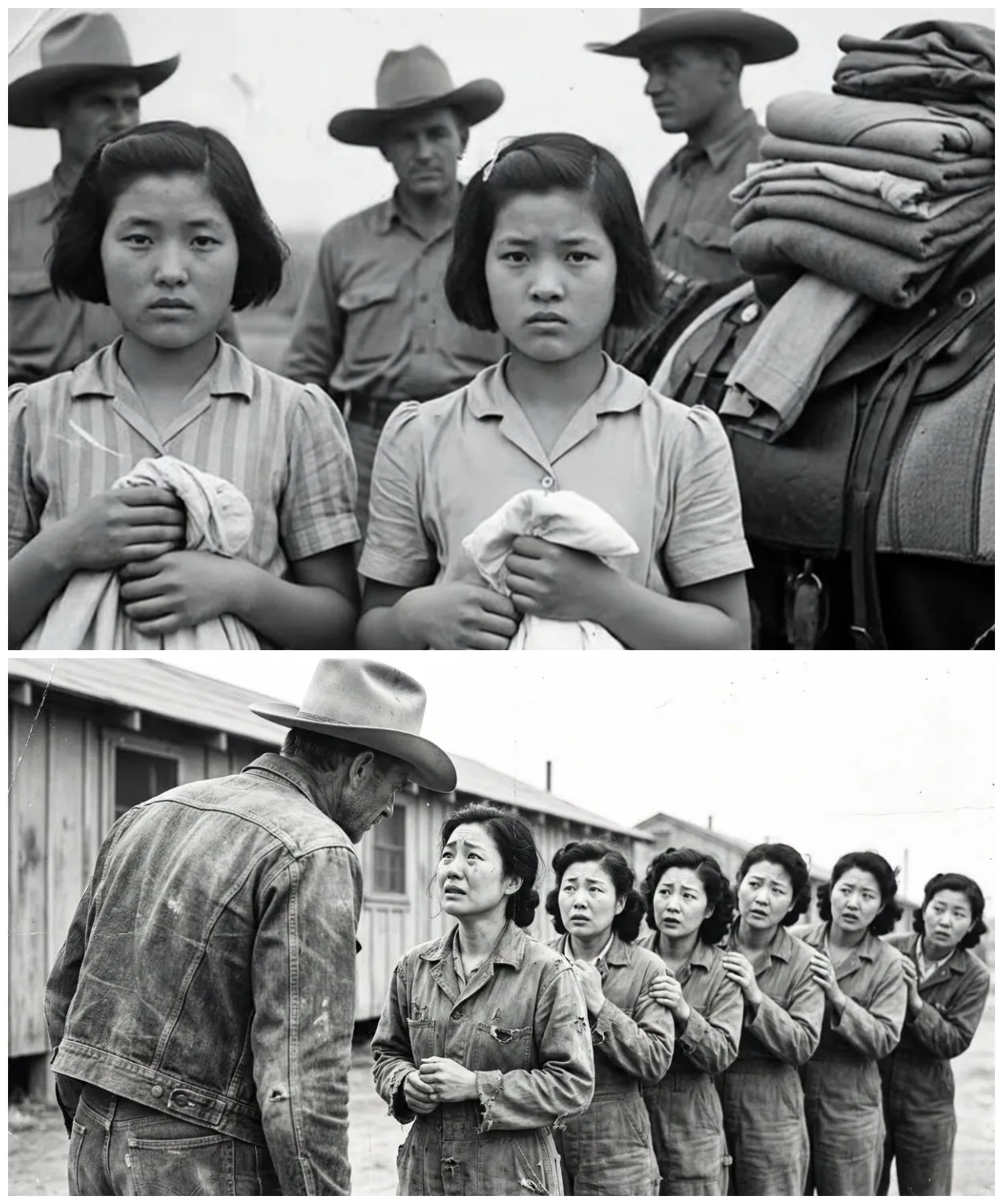
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked
They were told they would be stripped, punished, paraded. Instead, they were told to line up and handed dresses. The boots of the guards thudded softly against dry Texas soil as the sun climbed higher. A line of exhausted Japanese women stood barefoot in the dust, their eyes hollow, their uniforms torn. They had once […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 2
Another girl flinched when a medic approached her with a stethoscope. She covered her chest with both arms. Trembling, the medic froze, then slowly knelt down and placed the stethoscope against his own heart, tapping it twice, and smiled. She didn’t smile back, but she let him listen. One girl had a bruised wrist, deep […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 3
The field where they had learned to laugh again, the post where someone always left tea, the porch where banjos had played. And the men, the cowboys, the medics, the guards, they stood watching, hats in hand. Not victors, not jailers, just men changed, too. Because the truth was the war had ended long ago. […]
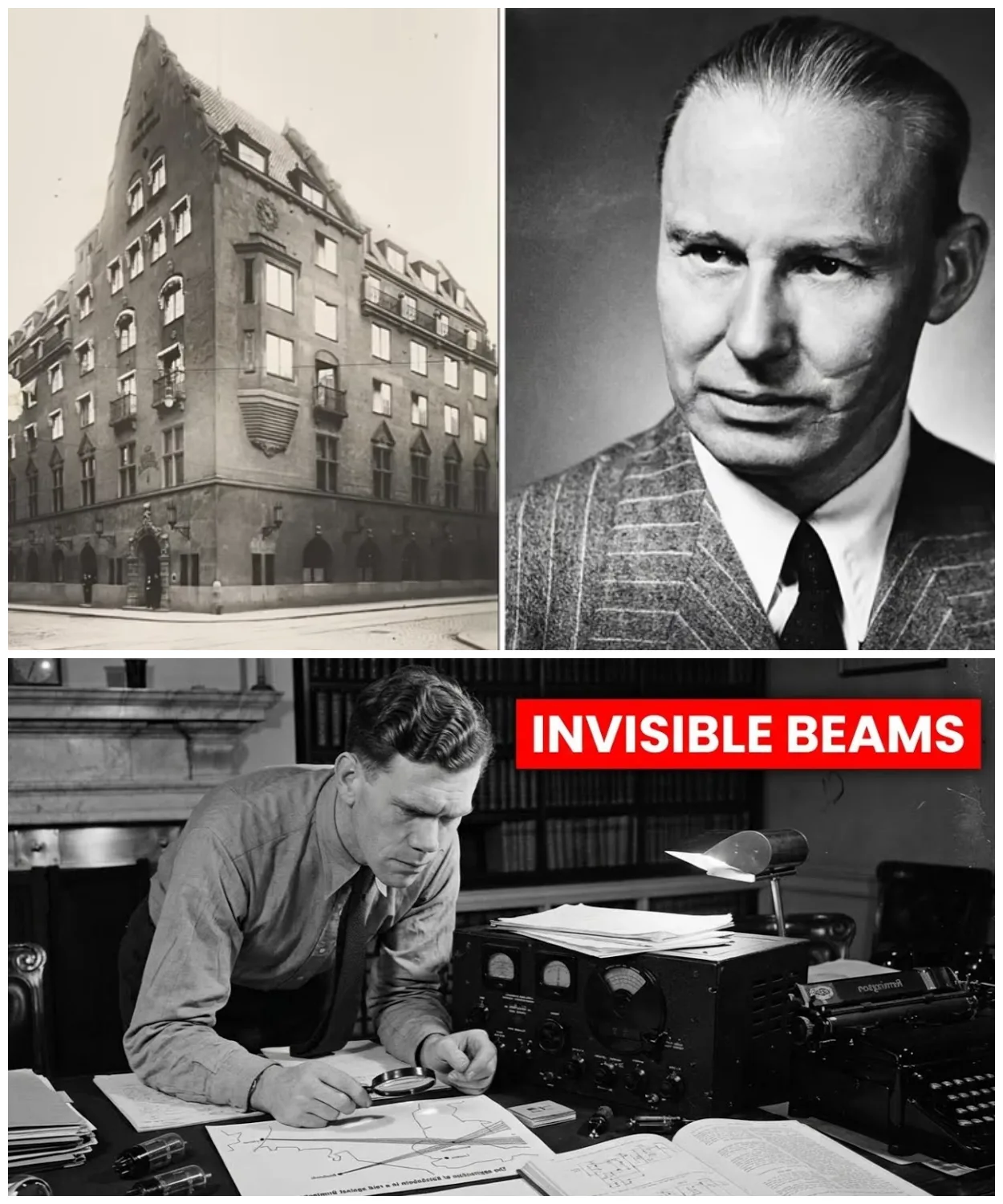
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio
June 21st, 1940. 10 Downing Street, the cabinet room. Reginald Victor Jones arrives 30 minutes late to a meeting already in progress. He’s 28 years old, the youngest person in the room by decades. Winston Churchill sits at the head of the table, 65, prime minister for 6 weeks. Around him, Air Chief Marshall Hugh […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio – Part 2
She memorizes them near photographic memory. Her September 1943 WTEL report identifies Colonel Max Waktell, gives precise operational details, maps planned launch locations from Britney to the Netherlands. When Jones inquires about the source, he’s told only one of the most remarkable young women of her generation. Rouso is arrested in April 1944. Survives three […]
End of content
No more pages to load













