When a shocking crime collides with complex questions of mental health and medication, the result is often a courtroom reckoning that extends far beyond the individuals involved.
That’s the dynamic now unfolding around Nick Reiner, son of celebrated Hollywood director Rob Reiner, following the killing of his parents—a tragedy that has stunned the entertainment world and sparked debate among psychiatrists, legal analysts, and the public.
In a widely discussed video response, Dr.
Yseph Whituring, a board-certified psychiatrist and drug safety expert who previously worked at the FDA, analyzes claims that Reiner’s actions may have been driven not purely by mental illness, but potentially by psychiatric medications—and their changes—administered in the weeks before the incident.
The conversation touches raw nerves: schizophrenia diagnoses, high-end rehab protocols, antipsychotic side effects, and the legal distinction between insanity defenses and involuntary intoxication due to prescribed drugs.
It’s a hard topic.
But it’s one that demands clarity, not sensationalism.
Here’s a grounded look at the issues Dr.Whituring raises, the defense strategies reportedly being considered, and the clinical and legal frameworks that will likely shape what happens in court.
A Reported Schizophrenia Diagnosis—and Skepticism
According to sources cited in media reports, Nick Reiner was diagnosed with schizophrenia and was under psychiatric care, receiving medications.
His behavior in the month before the murders was described by those sources as “erratic” and “dangerous.” He had reportedly been treated at a high-end Los Angeles rehab facility known for mental health specialization, with care costing up to $70,000 per month.
In the three to four weeks leading up to the killings, his medications were reportedly changed due to worsening behavior—and, per sources, the changes “weren’t right,” prompting further adjustments that allegedly failed to stabilize him.
Dr.Whituring’s first reaction: he’s skeptical of a new-onset schizophrenia diagnosis at age 32 in a male with a documented history of substance abuse.
While schizophrenia can emerge at various ages, classic onset often occurs in late adolescence or early adulthood—late teens to early 20s—especially in men.
Substance use can complicate the clinical picture by inducing psychotic symptoms or exacerbating underlying vulnerabilities.
That doesn’t rule out schizophrenia—but it raises questions about differential diagnosis.
From a forensic perspective, the timing matters.
If erratic behavior appeared closely after initiating or changing psychiatric medications—especially antipsychotics—that temporal relationship becomes a central inquiry.
Was the behavior consistent with schizophrenia? Or did it align more with known adverse drug effects, including agitation and impulsivity?
Antipsychotics, Akathisia, and Violence Risk: The Clinical Controversy
If Reiner was treated for schizophrenia, he was likely prescribed an antipsychotic.
Modern antipsychotics (both first- and second-generation) can be effective for psychosis, but they are not benign.
A well-documented and deeply uncomfortable side effect is akathisia—a state of intense inner restlessness, agitation, and anxiety.
Patients often describe feeling “on edge,” unable to sit still, and emotionally volatile.
In rare but notable cases, severe akathisia has been associated with aggression, self-harm, and impulsive acts.
Dr.
Whituring points to drug safety literature and labeling that includes warnings about agitation, hostility, impulsivity, and suicidal ideation.
He mentions medications like aripiprazole (brand name Abilify) as examples where labels list mood and behavioral adverse events.
While “homicidal ideation” is not universally listed across all antipsychotics, the constellation of agitation, akathisia, aggression, and impaired judgment is sufficiently recognized to warrant caution—particularly during dose changes, initiation, polypharmacy, or interactions with substances.
The underlying mechanism of akathisia isn’t fully settled, but dopaminergic and serotonergic modulation in the central nervous system are implicated.
Clinically, akathisia demands prompt recognition and management—through dose adjustment, medication changes, or adjuncts (such as beta blockers or benzodiazepines in some protocols)—to avoid escalation.
Dr.
Whituring’s core claim is not that antipsychotics “cause” violence as a direct, common effect, but that their rare, severe side effects, especially akathisia, can place certain individuals at heightened risk for impulsive, disorganized actions.
That risk is compounded in the presence of substance use, sleep deprivation, and underlying psychiatric instability.
Substance Use and Diagnostic Gray Zones
Reports suggest that Reiner had a history of substance abuse, with some claims of past methamphetamine use.
Stimulant-induced psychosis is a well-known phenomenon—methamphetamine, cocaine, and even high-dose prescription stimulants can produce hallucinations and paranoid delusions, sometimes with bizarre or aggressive behavior.
Separating substance-induced psychosis from primary psychotic disorders (like schizophrenia) is a clinical challenge.
The DSM-5 provides criteria to differentiate them, but in practice, time course, toxicology, and longitudinal history are critical.
If illicit drugs were present around the time of the crime (as confirmed by toxicology), a defense strategy that relies on medication-induced impairment becomes more difficult.
Courts often view voluntary ingestion of illegal substances as undermining claims of involuntary intoxication.
Conversely, if the primary agents were prescribed medications, recently initiated or altered by clinicians, an involuntary intoxication defense—where a defendant argues that a prescribed drug caused a state that negated criminal intent—may be considered.
Dr.
Whituring’s analysis leans toward a scenario where medication changes, possibly layered upon a vulnerable neuropsychiatric state, precipitated a destabilizing adverse reaction.
Whether that holds up in court depends on documentary evidence: medication logs, dose changes, clinical notes, nursing observations, pharmacy records, and testimony from clinicians, family, and witnesses.
Insanity vs.
Involuntary Intoxication: Two Legal Frameworks
The legal discourse around this case reportedly involves a plea of Not Guilty by Reason of Insanity (NGRI).
In many jurisdictions, NGRI relies on standards derived from the M’Naghten rule or similar tests: at the time of the act, due to a mental disease or defect, the defendant either did not understand the nature and quality of the act, or did not know it was wrong.
If the defense asserts schizophrenia as the underlying mental disease, NGRI becomes the primary path.
Alternatively, if prescribed medications (and their documented adverse effects) are central to the argument, the defense may emphasize involuntary intoxication: that a physician-prescribed agent caused a state of impaired capacity without the defendant’s volition.
Involuntary intoxication can function similarly to insanity defenses when it negates mens rea (criminal intent) or the capacity to appreciate wrongfulness.
Dr.
Whituring’s view is nuanced: he doubts new-onset schizophrenia at 32, favors an adverse drug reaction theory, and thus suggests involuntary intoxication could be viable if records corroborate medication-related destabilization.
He also notes that if illicit drugs are found in toxicology, that defense weakens substantially.
Historical comparisons—like John Hinckley Jr.’s NGRI after the Reagan shooting—are imperfect but relevant.
Hinckley spent years in a psychiatric facility and was released only after clinical evaluations deemed him no longer dangerous.
NGRI is not a “walk free” card; it redirects punishment toward treatment, often for long durations under strict conditions.
What Forensic Psychiatrists Will Look For
In constructing a psychiatric defense—or rebutting one—both sides will examine granular detail:
- Baseline behavior: Was there a prior history of violence? What was Reiner’s typical affect and impulse control outside periods of intoxication or instability?
- Timeline of medication changes: Exact dates, dosages, titration schedules, indications, side effects reported, and clinical responses.
Were akathisia or agitation documented?
- Clinical notes from the facility: Nursing shift notes, physician progress notes, crisis interventions, warnings to family, leave approvals for social events, and any “watch” status.
- Family and witness testimony: Observations that “he seemed different,” “out of his head,” “strange,” “hotheaded,” or “zoned out.” Eyewitness accounts at social events, such as the reported holiday party, will be central.
- Toxicology: UDS (urine drug screen), blood levels of prescribed medications, and detection of illicit substances.
- Environmental context: Sleep, stress, interpersonal conflict, agitation triggers, and any known medication interactions.
If medical sources indicate doctors were concerned that medication changes worsened symptoms—and if facility documentation shows efforts to adjust and stabilize without success—that evidence substantially bolsters an involuntary intoxication angle.
If medical notes instead support a progressive psychotic disorder with persistent symptoms independent of medication changes, the schizophrenia/NGRI case becomes more likely.
Akathisia in the Real World: A Clinical Cautionary Tale
Akathisia is a word most non-clinicians haven’t heard, but many have seen its manifestations.
Patients pace, rock, clench, and report unbearable inner tension.
Some describe a sense of “being driven” by an internal motor.
It is not mere anxiety; it is a distinct, physiologically rooted syndrome.
Left untreated, it can contribute to catastrophic outcomes—self-harm, aggression, or desperate, irrational acts.
Dr.
Whituring cites cases where drug-induced psychosis or severe akathisia precipitated tragic violence, including a highly publicized case involving an SSRI (an antidepressant) and a father who killed his son while in a state later described as drug-induced psychosis.
While such outcomes are rare, they underline why medication changes—especially in unstable patients—require close monitoring, conservative titration, and contingency planning.
A key clinical safeguard is early recognition.
Patients and families should be educated to report restlessness, agitation, insomnia, sudden irritability, or a “crawling out of my skin” sensation immediately.
Clinicians should respond rapidly with dose adjustments or medication switches, rather than treating through the symptoms without reassessment.
Public Perception vs.
Clinical Reality
There’s a temptation, in sensational cases, to reach for simple narratives: “schizophrenia made him do it,” or “the drugs made him do it.” Real life rarely obliges such clarity.
Comorbidity—coexisting conditions—is the rule rather than the exception.
A patient might have a vulnerability to psychosis, compounded by stress, worsened by substance use, destabilized by medication changes, and ultimately pushed into crisis by a perfect storm of factors.
That uncertainty is why courts rely on expert testimony, records, and cross-examination, rather than popular impressions or online speculation.
It’s also why clinicians push for precision in diagnosis: Is this schizophrenia? Schizoaffective disorder? Substance-induced psychotic disorder? Bipolar spectrum with psychotic features? Each diagnosis drives different treatment choices, risks, and legal interpretations.
Dr.
Whituring’s skepticism about a late schizophrenia diagnosis is reasonable insofar as it demands evidence.
It does not rule it out.
Some cases do present late.
Some patients mask symptoms for years.
The clinical record will be decisive, not the calendar alone.
The Reported Party Behavior: A Clue or a Rorschach?
Media accounts reference a holiday party where Reiner allegedly argued with his father and acted “in another world.” In isolation, an argument proves nothing.
In context—days or weeks of escalating agitation, medication changes, documented physician worry, sleep disturbance, and impulsivity—those observations may fit a pattern consistent with akathisia or drug-induced behavioral destabilization.
Witness testimony about demeanor (“zoned out,” “out of his head”) will carry weight.
But it must be mapped onto the clinical timeline and toxicology data to do more than color the narrative.
What the Jury Will Hear
If the defense pursues NGRI, jurors will hear psychiatric experts testify about mental disease and capacity at the time of the act: Did he understand the nature and quality of what he was doing, or that it was wrong? If the defense emphasizes involuntary intoxication, experts will focus on whether prescribed medications produced a state rendering him incapable of forming the requisite criminal intent.
The prosecution will likely emphasize agency: prior planning, concealment, flight, or efforts to avoid detection—behaviors often used to argue that the defendant knew the act was wrong.
They may also highlight any presence of illicit substances, contradictory witness statements, or behavior inconsistent with psychosis.
If facility records show clinicians warned of risks and adjusted meds responsibly, the prosecution may argue the adverse-effect claim is speculative.
The defense, conversely, will point to clinical records, physician notes, nurse observations, and family statements indicating dramatic changes after medication alterations.
They’ll argue that timing, intensity, and character of symptoms point away from longstanding psychosis and toward drug-induced destabilization.
If doctors documented that “the meds weren’t right,” that phrase becomes more than anecdote—it becomes evidentiary scaffolding.
A Painful Case with Broader Implications
Whatever the court decides, this case spotlights a broader medical reality: psychiatric medications save lives, but they require vigilant stewardship.
Antipsychotics, antidepressants, mood stabilizers, and anxiolytics can be transformative when carefully matched to diagnosis and closely monitored.
But dose changes and drug interactions—especially in patients with comorbid substance use—can detonate in unpredictable ways.
For families, the lesson is heartbreaking but practical:
- Track medication changes meticulously.
- Report early warning signs of agitation or akathisia.
- Advocate for slow titration and regular follow-up.
- Ensure coordinated care among prescribers, therapists, and facilities.
- Demand clear documentation and responsive adjustments when symptoms surge.
For clinicians, the case is a reminder to differentiate primary psychosis from substance-induced states rigorously, to screen for akathisia routinely, and to treat adverse effects as medical emergencies rather than background noise.
For the legal system, the challenge is to stitch together a narrative from clinical fragments and human testimony, resisting both moral panic and naive absolution.
Where Dr.
Whituring Lands—and What Remains Unknown
Dr.
Whituring’s analysis is cautious but pointed: he doubts a clean schizophrenia narrative at age 32 with this history, leans toward medication-induced destabilization, and suggests that an involuntary intoxication defense is plausible if records back it up.
He acknowledges that insanity (NGRI) is the likely legal vehicle if the defense formalizes schizophrenia as the disease at issue.
He also notes the heavy hinge on toxicology—illicit drugs would complicate or undercut the involuntary intoxication claim significantly.
Ultimately, the question is one courts labor over in every such case: What was happening in the defendant’s mind at the time of the act, and why?
The answer will not come from televised analysis alone.
It will come from patient files, pharmacy logs, clinical notes, toxicology reports, and hours of testimony.
It will come from the messy, imperfect process of sorting human suffering into legal categories.
And while the law must make a determination, the human story behind it remains irreducibly tragic—parents who tried to help, clinicians who tried to stabilize, a son whose life became a battleground of diagnosis, treatment, relapse, and risk.
In the end, the case may redefine nothing and teach everything: that psychiatric care is as delicate as it is essential, that side effects can be as dangerous as symptoms, and that the line between illness and intent is not always as easy to draw as we wish it to be.
News

A Single Dad Helped a Deaf Woman at the Airport — He Had No Idea Her Daughter Was a CEO!..
I was standing in the middle of one of the busiest airports in the country, surrounded by hundreds of people rushing to their gates, dragging suitcases, staring at their phones, completely absorbed in their own little worlds. And in the middle of all that chaos, there was this older woman, elegantly dressed, silver hair pinned […]
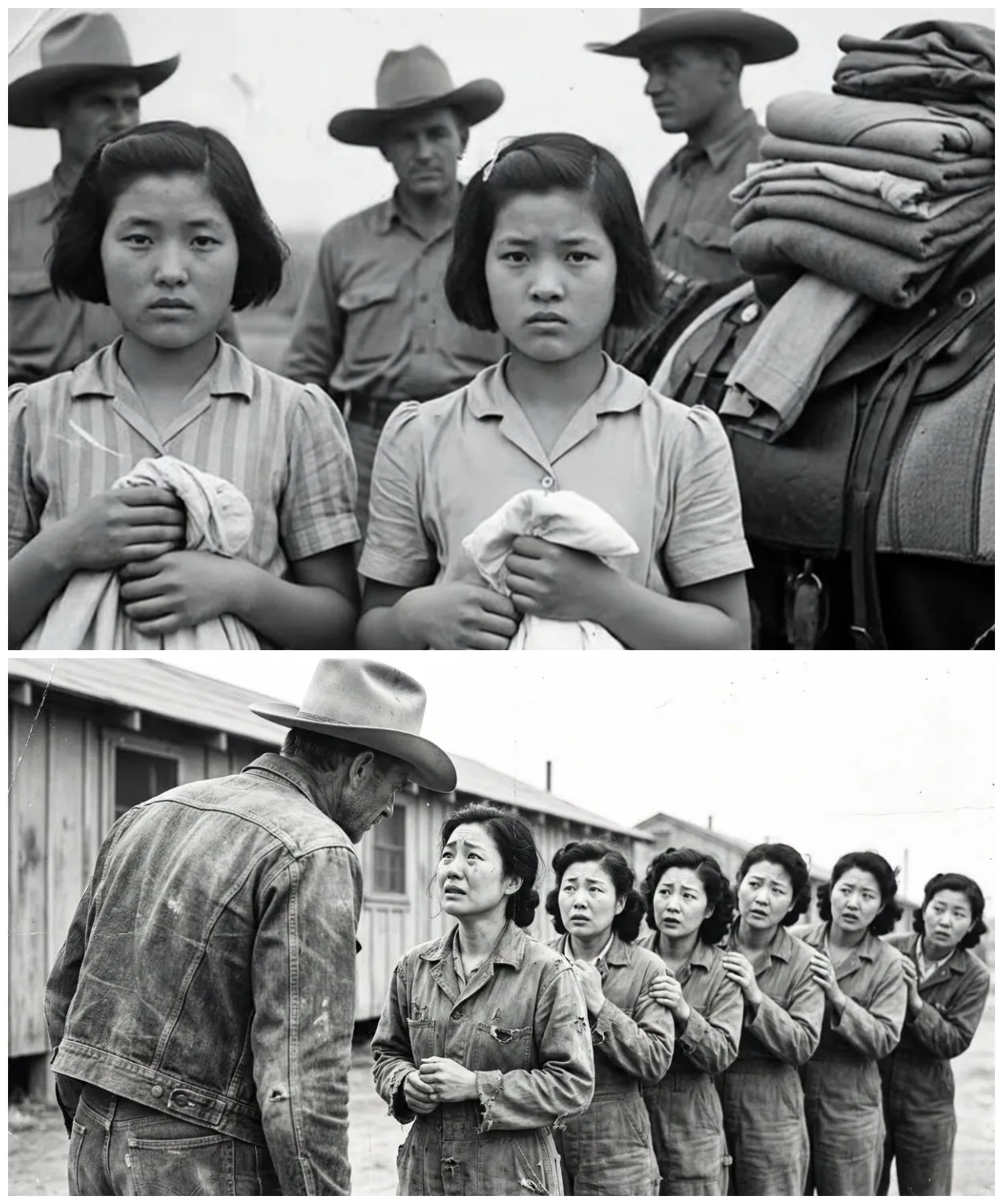
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked
They were told they would be stripped, punished, paraded. Instead, they were told to line up and handed dresses. The boots of the guards thudded softly against dry Texas soil as the sun climbed higher. A line of exhausted Japanese women stood barefoot in the dust, their eyes hollow, their uniforms torn. They had once […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 2
Another girl flinched when a medic approached her with a stethoscope. She covered her chest with both arms. Trembling, the medic froze, then slowly knelt down and placed the stethoscope against his own heart, tapping it twice, and smiled. She didn’t smile back, but she let him listen. One girl had a bruised wrist, deep […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 3
The field where they had learned to laugh again, the post where someone always left tea, the porch where banjos had played. And the men, the cowboys, the medics, the guards, they stood watching, hats in hand. Not victors, not jailers, just men changed, too. Because the truth was the war had ended long ago. […]
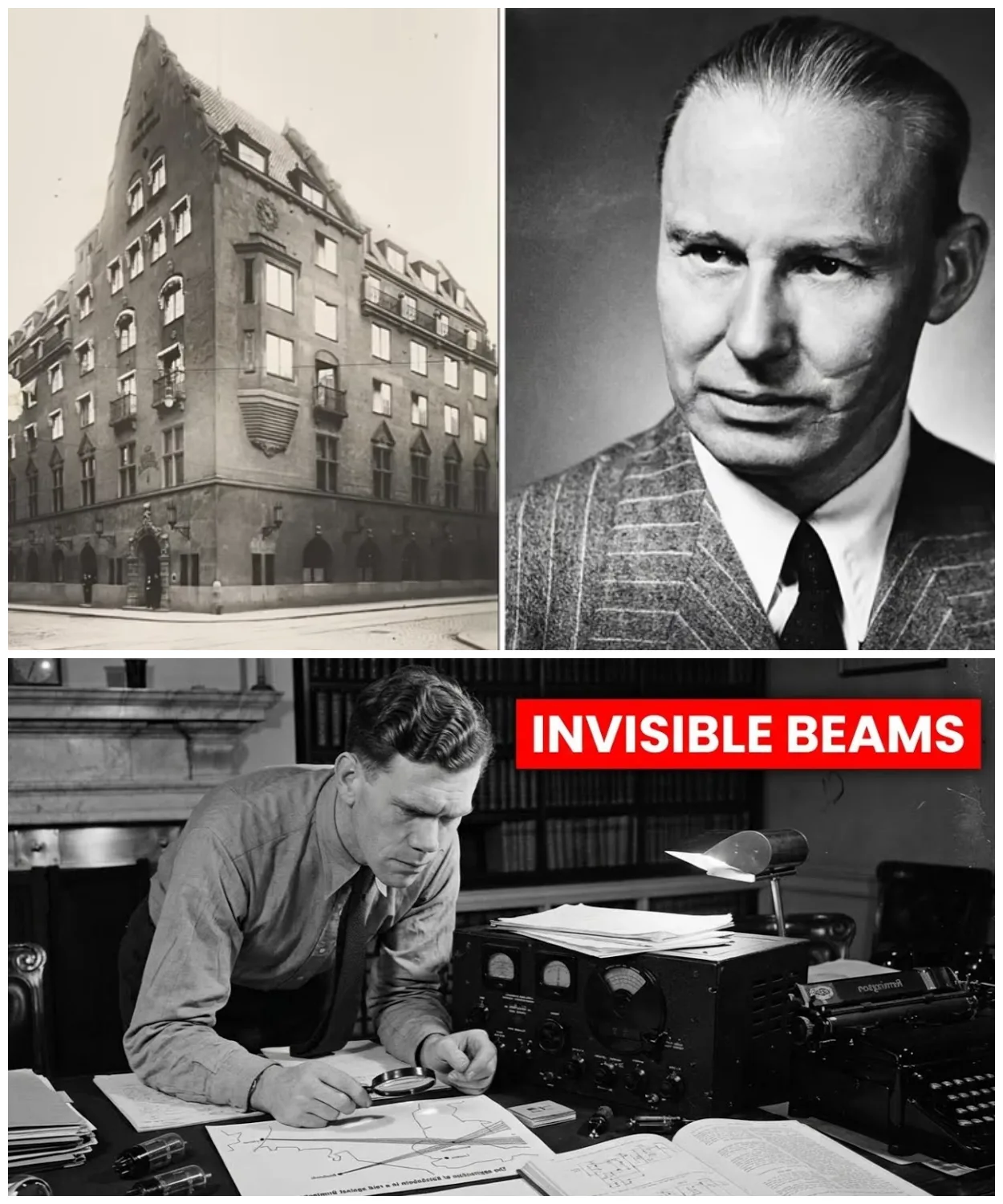
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio
June 21st, 1940. 10 Downing Street, the cabinet room. Reginald Victor Jones arrives 30 minutes late to a meeting already in progress. He’s 28 years old, the youngest person in the room by decades. Winston Churchill sits at the head of the table, 65, prime minister for 6 weeks. Around him, Air Chief Marshall Hugh […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio – Part 2
She memorizes them near photographic memory. Her September 1943 WTEL report identifies Colonel Max Waktell, gives precise operational details, maps planned launch locations from Britney to the Netherlands. When Jones inquires about the source, he’s told only one of the most remarkable young women of her generation. Rouso is arrested in April 1944. Survives three […]
End of content
No more pages to load