The boy stands in the intake line at Camp Aliceville, Alabama, with his chin locked forward like a statue.
The American guard asks him to turn his head left.
Nothing.
Turn your head right.
Still nothing.
The boy’s eyes shift, but his neck does not move even a fraction of an inch.
The guard writes something down, but the medic who sees it next does not write anything.
He just stares because what he is looking at does not match what a 17-year-old spine should be able to do.
The boy who cannot turn his head has a name, but no one at Camp Aliceville knows it yet.
It is late 1944 and the war in Europe is turning against Germany with brutal speed.

Thousands of German prisoners of war are being shipped across the Atlantic to camps inside the United States, far from bombed cities and collapsing fronts.
Camp Aliceville in Alabama is one of dozens of facilities designed to hold enemy soldiers until the war ends.
Most prisoners arrive exhausted, hungry, and confused.
But they arrive walking, talking, and turning their heads when someone calls their name.
This boy does not.
His name is Becker, though some records spell it Klouse, and he is 17 years old when he steps off the transport truck in front of the camp medical building.
He is thin, pale, and quiet.
But those traits are common among boys pulled from the final months of fighting on the Western Front.
What is not common is the way he holds his entire upper body rigid, as if his spine is fused from the base of his skull down to his shoulder blades.
When the intake officer asks him a question from the left side, Becker does not turn his head.
He rotates his entire torso like a wooden mannequin.
The officer assumes it is defiance.
The medic standing behind him assumes it is something much worse.
They bring Becker into the camp clinic within the first hour.
The head physician, Dr.
Raymond Callaway, is a civilian contracted by the war department, and he has seen broken bones, infected wounds, and advanced tuberculosis in prisoners arriving from Europe.
But he has never seen a boy whose neck refuses to move in any direction.
Callaway orders Becker to sit on the exam table and he begins the assessment with the most basic test.
Turn your head to the left.
Becker does not move.
Turn it to the right.
Still nothing.
The boy’s eyes flick toward the doctor, but his head remains locked in a perfectly straight forward position as if his skull is bolted to his spine.
Callaway places his hands on either side of Becker’s jaw and applies gentle pressure, testing whether the joint is simply stiff or whether something structural is preventing motion.
The moment he pushes, Becker inhales sharply through his teeth and his eyes water.
Callaway stops immediately.
He moves his hands to the back of the boy’s neck, feeling along the vertebrae, and what he finds makes him pull his assistant closer without saying a word.
The spine is not smooth.
There are hard ridges and uneven surfaces where the bone should be uniform.
The tissue around the upper vertebrae is swollen and knotted.
And when Callaway presses just below the base of the skull, Becker jerks forward and nearly vomits from the pain.
We are still in the camp clinic at Camp Aliceville.
Minutes after the first examination, and Dr.
Callaway is trying to understand what he just felt under Becker’s skin.
Dr.
Callaway steps back and looks at his assistant, nurse Helen Courtland, who has been writing notes on a clipboard.
He tells her to flag this case as urgent and to request an X-ray machine from the base hospital in Birmingham.
Camp Aliceville does not have the equipment to image bone structures in detail.
And without an X-ray, Callaway is working blind.
But even without the image, he already has a theory, and it is not a comforting one.
The boy’s neck is not stiff because of muscle strain or temporary inflammation.
The spine itself has been damaged, possibly fractured, and the body has tried to repair it by fusing the bones together in whatever position they were held during the injury.
Nurse Courtland asks the question that both of them are thinking.
How long has he been like this? Callaway does not know, but he guesses it has been months, maybe longer.
If the injury had happened recently, the pain would be sharper and the swelling more severe.
What Becker is showing looks like an old wound that healed incorrectly, which means he has been living with a locked neck for a significant portion of the war.
That raises another question that Callaway writes down in the margin of his notes.
If this boy could not turn his head, how did he fight? How did he survive combat, transport, and capture without being able to look left or right? The next step is to interview Becker directly, but there is a language problem.
Becker speaks German and very little English, and the camp interpreter is tied up processing a hundred other prisoners that same afternoon.
Callaway tries basic questions in slow English, using hand gestures to fill in the gaps.
Where were you hurt? Becker points vaguely at his neck.
When did it happen? Becker shrugs or tries to, but the motion is so restricted that it looks more like a tremor.
Callaway switches tactics and asks yes or no questions.
Did this happen in battle? Becker nods.
Did a vehicle hit you? Becker shakes his head, then winces because even that small motion sends a spike of pain down his upper back.
Callaway makes a note to revisit the interrogation once the interpreter is available.
But he also makes a second note, one that he does not share with nurse Courtland yet.
The boy is scared, not of the examination and not of the camp.
He is scared of what the doctor might find.
Three days pass and the X-ray equipment finally arrives from Birmingham along with a specialist who will change everything Becker thought he understood about his own body.
Three days later, the X-ray equipment arrives from Birmingham along with a radiologist named Lieutenant Paul Hendris, who sets up a portable unit in one of the camp storage buildings.
Becker is brought in under guard, though the guard quickly realizes there is no need for restraint.
The boy is cooperative, almost passive, and he follows every instruction without resistance.
Lie down on the table.
Stay still.
Do not move your head.
Becker does exactly what he is told and Hrix takes four images, front, back, left side, right side.
When the films are developed an hour later, Hrix does not wait for a formal meeting.
He walks directly to Dr.
Callaway’s office with the X-rays in hand and clips them onto the light box without saying a word.
Callaway stands up, moves closer, and stares at the images for nearly a full minute before he speaks.
The third and fourth cervical vertebrae, the bones that should allow the neck to rotate and flex, are fractured in multiple places.
But the fractures are not clean breaks.
They are compression fractures, the kind caused by a sustained vertical force, as if something extremely heavy pressed down on the top of Becker’s head and crushed the vertebrae from above.
What makes the images even more disturbing is the calcification.
The body has tried to repair the damage by laying down new bone tissue.
But because Becker never had access to proper medical care, the bones fused together in a crooked, uneven mass.
His third and fourth vertebrae are now essentially one solid block of malformed bone, which is why his neck cannot move.
The surrounding muscles have adapted by going into permanent spasm, which is why the tissue feels like stone when you press on it.
Hrix points to a shadow on the left side of the spine and says it looks like scar tissue from an old hematoma, meaning Becker also bled internally when the injury first occurred.
Callaway asks the question that has been gnawing at him since the first exam.
How is this boy still alive? Hrix does not have a medical answer, but he has a guess.
If the fracture had been even a few millimeters higher or deeper, it would have severed the spinal cord and Becker would have been paralyzed or killed instantly.
Instead, the fracture crushed the bones but left the cord intact, which means Becker kept all of his motor function below the neck.
He could walk, run, use his arms, and carry a rifle.
He just could not turn his head.
But that explanation does not satisfy Callaway because it does not explain how Becker survived the acute phase of the injury.
Compression fractures in the cervical spine are agonizingly painful and they usually require immediate immobilization and surgery.
Becker had neither.
He had no surgery, no traction, no stabilization.
And yet he walked out of whatever battlefield or transport vehicle he was in and kept going.
Callaway writes one word in his notes and underlines it twice.
Adrenaline.
The moment everyone has been waiting for finally arrives when the interpreter walks into the medical office and sits down across from the boy who survived the impossible.
The interpreter finally arrives on the fifth day, a German-speaking corporal named Eugene Faulk, who was born in Milwaukee to immigrant parents.
Faulk sits across from Becker in the medical office and begins the interview with simple questions to establish trust.
Where are you from? Becker says a small town near Dortmund.
How old are you? 17, almost 18.
When were you drafted? March of 1944.
Faulk takes his time and Callaway watches from the side of the room, letting the conversation unfold naturally.
Then Faulk asks the critical question.
What happened to your neck? Becker hesitates and for a moment it looks like he will refuse to answer, but then he starts talking slowly at first and Faulk translates sentence by sentence.
Becker was assigned to a panzer unit in France during the summer of 1944 shortly after the Allied invasion at Normandy.
He was not a tank driver or a gunner.
He was part of the ground crew, the soldiers who ran alongside the tanks and protected them from infantry attacks.
His unit was caught in an artillery barrage near the town of Phalet in August and Becker was crouched behind a halftrack when a shell landed less than 20 m away.
He does not remember the explosion itself, only the pressure.
He says it felt like a giant hand pressed down on the top of his head and shoved his spine into the ground.
When he woke up, he was lying on his side in a ditch and his neck would not move.
He could not lift his head and he could not turn it left or right.
The pain was so severe that he vomited twice and then passed out again.
When he woke the second time, the artillery barrage was over and most of his unit was dead or scattered.
Let us know in the comments where you are watching this from.
Are you in the United States, Germany, the United Kingdom, or somewhere else? If you want to dive even deeper into these untold stories, consider becoming a channel member.
You’ll get your name mentioned in the video, early access to videos, exclusive content, and direct input on which stories we cover next.
Join our inner circle of history keepers.
Becker’s story is about to get even more unbelievable because what happened next should not have been survivable.
Becker crawled out of the ditch and found two other soldiers from his company.
Both of them wounded but mobile.
They told him the regiment was retreating toward the Sen River, and if they did not move fast, they would be surrounded by Canadian forces.
Becker tried to stand and his legs worked, but his head stayed locked in place.
One of the soldiers, an older man named Datri, told him to hold his head with both hands while they walked so it would not flop around.
Becker did exactly that.
He held his own head steady with his hands pressed against his jaw and the base of his skull, and he walked 17 kilometers through French farmland to reach the fallback position.
We are now back in France in August of 1944 following Becker as he reaches the German fallback position with a broken neck and no medical help in sight.
Faulk pauses the translation and asks Becker a follow-up question.
Did you see a medic? Becker nods carefully and says he saw a medic the next day at a field hospital.
The medic told him his neck was broken, but there was nothing they could do.
There was no surgery available.
No hospital with the right equipment, and the regiment was moving again in 6 hours.
The medic gave Becker a roll of gauze, a wooden splint, and a handful of morphine tablets.
He told Becker to wrap the splint around his neck to keep it stable and to take the morphine when the pain was unbearable.
Then the medic moved on to the next patient.
Becker spent the next four months fighting, retreating, and surviving with a cervical spine that had been fractured and never repaired.
He wore the makeshift splint for 3 weeks until the gauze rotted and fell apart, and then he learned to manage without it.
He kept his head as still as possible, and he moved his entire upper body whenever he needed to look in a different direction.
His squadmates made jokes at first, calling him the statue and the wooden soldier.
But the joke stopped after the first time.
Becker took a rifle shot without turning his head.
He learned to aim using only his peripheral vision and his body rotation.
And he learned to sleep sitting up because lying down sent sharp pains through his skull.
The morphine ran out after 2 weeks and Becker never received more.
He managed the pain by staying in motion because standing still made him focus on the pressure in his neck and focusing on it made it worse.
He ate when food was available, which was not often, and he drank water from rivers and canteen shares.
His weight dropped, and his endurance suffered, but his neck stabilized in its fused position, and the acute pain gradually became a chronic ache that he could tolerate.
He never told his officers about the severity of the injury because admitting it would have meant being left behind and being left behind in a retreating German army in late 1944 often meant being captured, executed, or abandoned to die.
Becker’s war finally ends in November near the German border.
But his real test is just beginning.
Becker was finally captured in November near the German border when his unit ran out of ammunition and surrendered to an American patrol.
The American soldiers searched him, took his rifle, and marched him to a temporary holding area with 40 other prisoners.
No one noticed his neck during the initial processing because Becker had learned to move carefully and avoid drawing attention.
He was loaded onto a truck, then a train, then a ship, and finally another train that brought him to Alabama.
It was not until the intake line at Camp Aliceville that an American guard saw the way Becker held his head and flagged him for medical review.
Dr.
Callaway listens to the full translation and then asks Faulk to clarify one detail.
How much pain is Becker in right now? Faulk asks and Becker pauses before answering.
He says the pain is always there, but it is not as bad as it was in August.
He describes it as a heavy weight pressing down on the top of his head and a burning sensation that runs from the base of his skull down to his shoulder blades.
If he turns his torso too quickly, the burning becomes sharp and sometimes his vision goes white for a few seconds.
If he tries to tilt his head up or down, his hands start to go numb.
Callaway writes all of this down and then asks one more question through Faulk.
Do you want us to try to fix it? Becker looks at Callaway for the first time during the interview and his expression is hard to read.
He does not say yes and he does not say no.
He says, “Can you?” We are back at Camp Aliceville where an American doctor is about to make a decision that will change the rules for how prisoners of war are treated.
Dr.
Callaway brings the case to the camp’s chief medical officer and requests authorization to transfer Becker to a military hospital with a neurosurgery department.
The request is unusual because prisoners of war typically receive only basic medical care and complex surgeries are reserved for allied personnel.
But Callaway argues that Becker’s case falls under the Geneva Convention’s mandate to provide necessary medical treatment to prisoners.
And he emphasizes that the boy’s injury is life-threatening.
If the fused vertebrae shift even slightly, they could compress the spinal cord and cause permanent paralysis or death.
The chief medical officer approves the transfer, but with a condition.
The surgery must be approved by an army neurosurgeon and Becker must consent in writing.
Faulk explains the situation to Becker in German, and Becker listens without interrupting.
Faulk tells him the surgery would involve cutting into the back of his neck, removing the malformed bone, and possibly inserting metal hardware to stabilize the spine.
The recovery would take months, and there is no guarantee it would restore full range of motion.
There is also a risk of complications including infection, bleeding, and paralysis.
Becker asks one question.
If I do not have the surgery, what happens? Faulk translates Callaway’s answer.
You will live with the pain and eventually the fused bones might press on your spinal cord and kill you.
It could happen in 5 years or it could happen tomorrow.
Becker signs the consent form the next day.
If you are enjoying this story and want more untold accounts from World War II prisoners of war, make sure to subscribe to the channel.
We are bringing you stories that most history books never covered.
Becker is about to become one of the first German prisoners of war to receive major spinal surgery on American soil, and no one knows if he will survive it.
Becker leaves Camp Aliceville behind and enters a world of surgical precision that does not care whether he is a prisoner or a patient.
Becker is transferred to Lawson General Hospital in Atlanta, Georgia, one of the largest military medical facilities in the southern United States.
The hospital has a dedicated neurosurgery unit staffed by army doctors who trained at some of the best medical schools in the country and they have been treating combat injuries since the early years of the war.
Becker arrives in early December 1944 and he is assigned to a ward with other patients awaiting surgery.
Most of them are American soldiers with shrapnel wounds, amputations and traumatic brain injuries.
Becker is the only prisoner of war in the unit, and he is the only patient whose injury is 4 months old and still untreated.
The lead surgeon, Major Thomas Elwood, reviews Becker’s X-rays and medical history before meeting him in person.
Elwood has performed dozens of spinal surgeries during the war, but most of them involved acute injuries that were treated within days or weeks of the trauma.
Becker’s case is different because the bones have already fused and reversing that process will require removing calcified tissue and manually separating vertebrae that the body has tried to weld together.
Elwood describes the procedure to his surgical team as controlled demolition because the goal is to break apart the malformed bone without damaging the spinal cord that runs directly underneath it.
Elwood meets with Becker two days before the surgery and uses an interpreter to explain the risks one more time.
Becker listens, nods carefully, and says he understands.
Elwood asks him why he is willing to take the risk, and Becker gives an answer that the interpreter translates word for word.
I have been holding my head in place with my hands for 4 months.
I want to use my hands for something else.
It is December 14th, 1944, and a German boy is about to receive 6 hours of American surgery that will either save his life or end it.
The operation takes place on December 14th, 1944, and it lasts nearly 6 hours.
Becker is placed under general anesthesia and positioned face down on the operating table with his head secured in a metal frame.
Major Elwood makes an incision down the back of Becker’s neck, cutting through skin, muscle, and connective tissue to expose the damaged vertebrae.
The moment the bone is visible, Elwood sees the extent of the problem.
The third and fourth cervical vertebrae are encased in a thick layer of calcified tissue, and the joint between them has completely disappeared.
The bones have fused at a slight angle, which is why Becker’s head sits tilted slightly forward.
Elwood uses a surgical drill to carefully remove the calcified overgrowth, working in small increments to avoid slipping and cutting into the spinal cord.
The process is slow and painstaking, and twice during the procedure, Elwood pauses to let his hands rest because the precision required is exhausting.
Once the excess bone is cleared away, Elwood assesses the underlying vertebrae and finds that the fractures have healed, but in a misaligned position, he makes the decision to leave the healed fractures in place rather than risk destabilizing the spine further, and instead he focuses on restoring mobility by creating space between the fused bones.
Using a combination of drills, chisels, and manual pressure, Elwood separates the third and fourth vertebrae by inserting a thin metal spacer between them.
The spacer is designed to hold the bones apart while the surrounding tissue heals, and it will remain in Becker’s neck permanently.
Once the spacer is in place, Lwood tests the range of motion by gently moving Becker’s head from side to side.
The movement is limited, but it is present, which means the surgery has achieved its primary goal.
Elwood closes the incision with sutures, and Becker is moved to the recovery ward.
Becker wakes up in the recovery ward and immediately learns that surviving the surgery was only the beginning of his fight.
Becker wakes up in the recovery ward with his neck wrapped in bandages and his head immobilized in a rigid brace.
The pain is immediate and severe, worse than anything he felt during the original injury, and he is given morphine to manage it.
For the first 3 days, he is not allowed to move his head at all, and nurses adjust his position every few hours to prevent pressure sores.
On the fourth day, a physical therapist named Lieutenant Sarah Brennan visits his bedside and explains the rehabilitation process.
Brennan tells Becker that the goal is to gradually restore range of motion without displacing the metal spacer or damaging the healing tissue.
The process will take weeks, possibly months, and it will be painful.
Becker will start with passive exercises where Brennan moves his head for him and eventually progress to active exercises where he moves his own head under supervision.
Becker listens to the translation and asks one question.
Will I be able to turn my head all the way? Brennan is honest.
Probably not all the way, but more than you can now.
The rehabilitation is brutal.
Every session involves stretching scar tissue that has been locked in place for months, and every stretch feels like Becker’s neck is being torn apart from the inside.
He vomits twice during the first week of therapy and once he passes out from the pain, but he keeps going because the alternative is returning to Camp Aliceville with a neck that still does not move.
By the third week, Becker can turn his head 15° to the left and 20° to the right.
By the sixth week, he can look over his shoulder.
By the eighth week, he can tilt his head up and down without his hands going numb.
Major Elwood visits Becker during the final week of rehabilitation, and performs a follow-up exam.
He measures Becker’s range of motion, tests his reflexes, and reviews a new set of X-rays.
The metal spacer is still in place, and the surrounding bone shows signs of healthy healing.
Elwood tells Becker that the surgery was a success, and that he has regained approximately 60% of his normal neck mobility.
Becker will never have full range of motion and he will likely experience chronic pain for the rest of his life, but he will be able to live without holding his head in place with his hands.
Becker asks Elwood one question before he leaves.
Why did you do this for me? Elwood pauses, then gives an answer that the interpreter translates carefully.
Because you are a patient and I am a doctor.
The war does not change that.
Becker’s story is rare, but the system that saved him was not, and the numbers prove it.
The story of Becker is rare, but the statistics behind it are not.
During World War II, more than 11 million soldiers became prisoners of war across all theaters of combat.
Germany held approximately 3 and a half million Allied prisoners, while the Allies held approximately 4 million German and Italian prisoners.
The United States alone held over 400,000 German prisoners in camps scattered across the country, and Camp Aliceville in Alabama was one of the largest, housing up to 6,000 men at its peak.
Medical care for prisoners of war varied widely depending on the capturing nation and the stage of the war.
The Geneva Convention of 1929 required all nations to provide necessary medical treatment to prisoners, but enforcement was inconsistent.
The United States and the United Kingdom generally adhered to the convention, and many prisoners received surgeries and treatments that would have been impossible in their home countries due to resource shortages.
Germany and Japan were far less consistent, and millions of Soviet prisoners in German custody died from neglect, starvation, and untreated injuries.
Spinal injuries were among the most feared wounds of the war because they often resulted in permanent paralysis or death.
The survival rate for cervical spine fractures in combat conditions was estimated at less than 30%.
and most of those who survived the initial injury died within weeks due to infection or secondary complications.
Becker’s survival with a fractured cervical spine for 4 months without surgery is medically extraordinary and his successful treatment by American military surgeons reflects the advanced state of neurosurgery in the United States during the 1940s.
More than 70,000 German prisoners of war were treated in American military hospitals during the war and thousands of those treatments involved complex surgeries that saved lives and restored function.
Becker was one of those thousands and his case became part of the medical literature on spinal trauma, though his name was changed in the published reports to protect his privacy.
News

A Single Dad Helped a Deaf Woman at the Airport — He Had No Idea Her Daughter Was a CEO!..
I was standing in the middle of one of the busiest airports in the country, surrounded by hundreds of people rushing to their gates, dragging suitcases, staring at their phones, completely absorbed in their own little worlds. And in the middle of all that chaos, there was this older woman, elegantly dressed, silver hair pinned […]
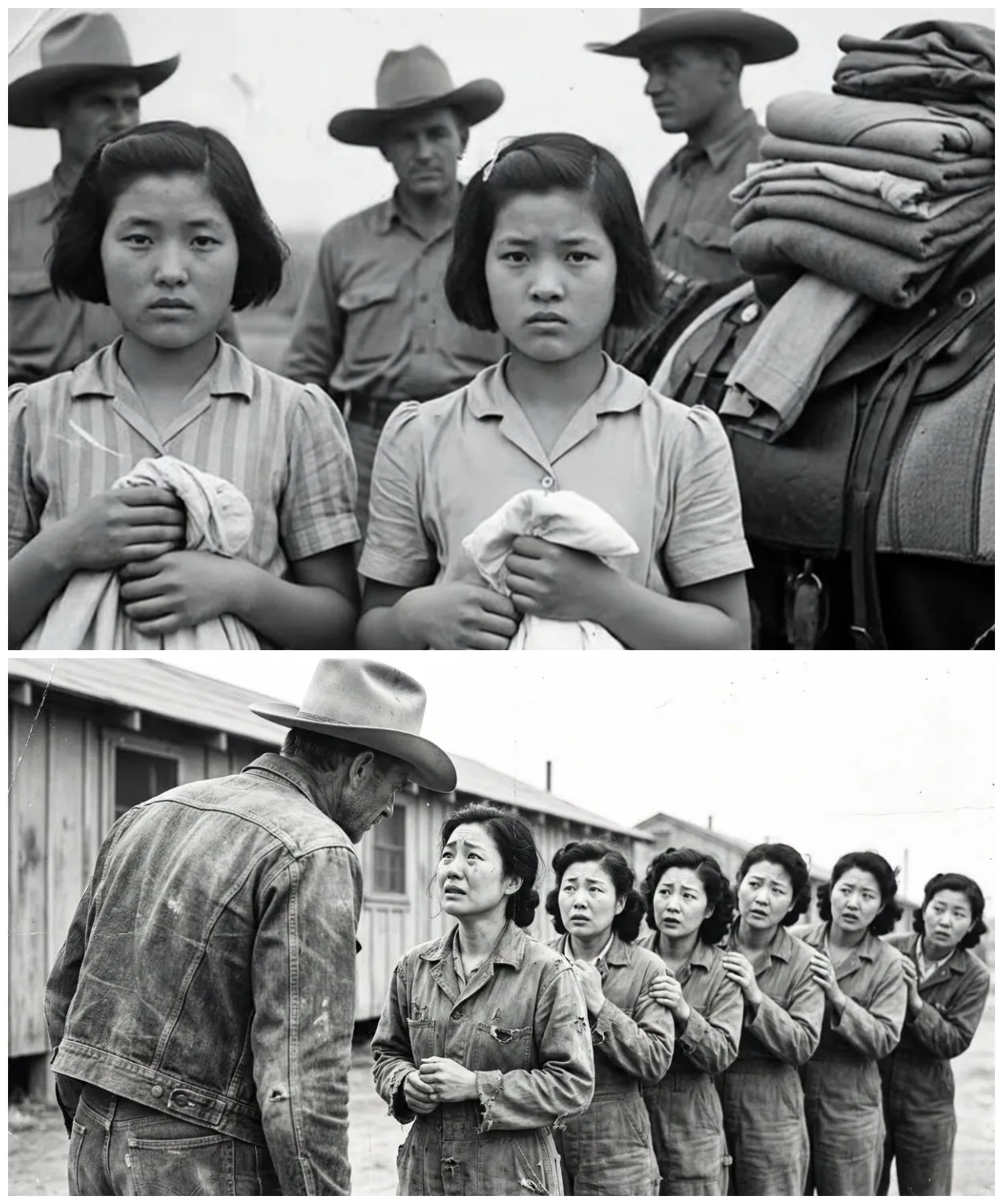
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked
They were told they would be stripped, punished, paraded. Instead, they were told to line up and handed dresses. The boots of the guards thudded softly against dry Texas soil as the sun climbed higher. A line of exhausted Japanese women stood barefoot in the dust, their eyes hollow, their uniforms torn. They had once […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 2
Another girl flinched when a medic approached her with a stethoscope. She covered her chest with both arms. Trembling, the medic froze, then slowly knelt down and placed the stethoscope against his own heart, tapping it twice, and smiled. She didn’t smile back, but she let him listen. One girl had a bruised wrist, deep […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 3
The field where they had learned to laugh again, the post where someone always left tea, the porch where banjos had played. And the men, the cowboys, the medics, the guards, they stood watching, hats in hand. Not victors, not jailers, just men changed, too. Because the truth was the war had ended long ago. […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio
June 21st, 1940. 10 Downing Street, the cabinet room. Reginald Victor Jones arrives 30 minutes late to a meeting already in progress. He’s 28 years old, the youngest person in the room by decades. Winston Churchill sits at the head of the table, 65, prime minister for 6 weeks. Around him, Air Chief Marshall Hugh […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio – Part 2
She memorizes them near photographic memory. Her September 1943 WTEL report identifies Colonel Max Waktell, gives precise operational details, maps planned launch locations from Britney to the Netherlands. When Jones inquires about the source, he’s told only one of the most remarkable young women of her generation. Rouso is arrested in April 1944. Survives three […]
End of content
No more pages to load