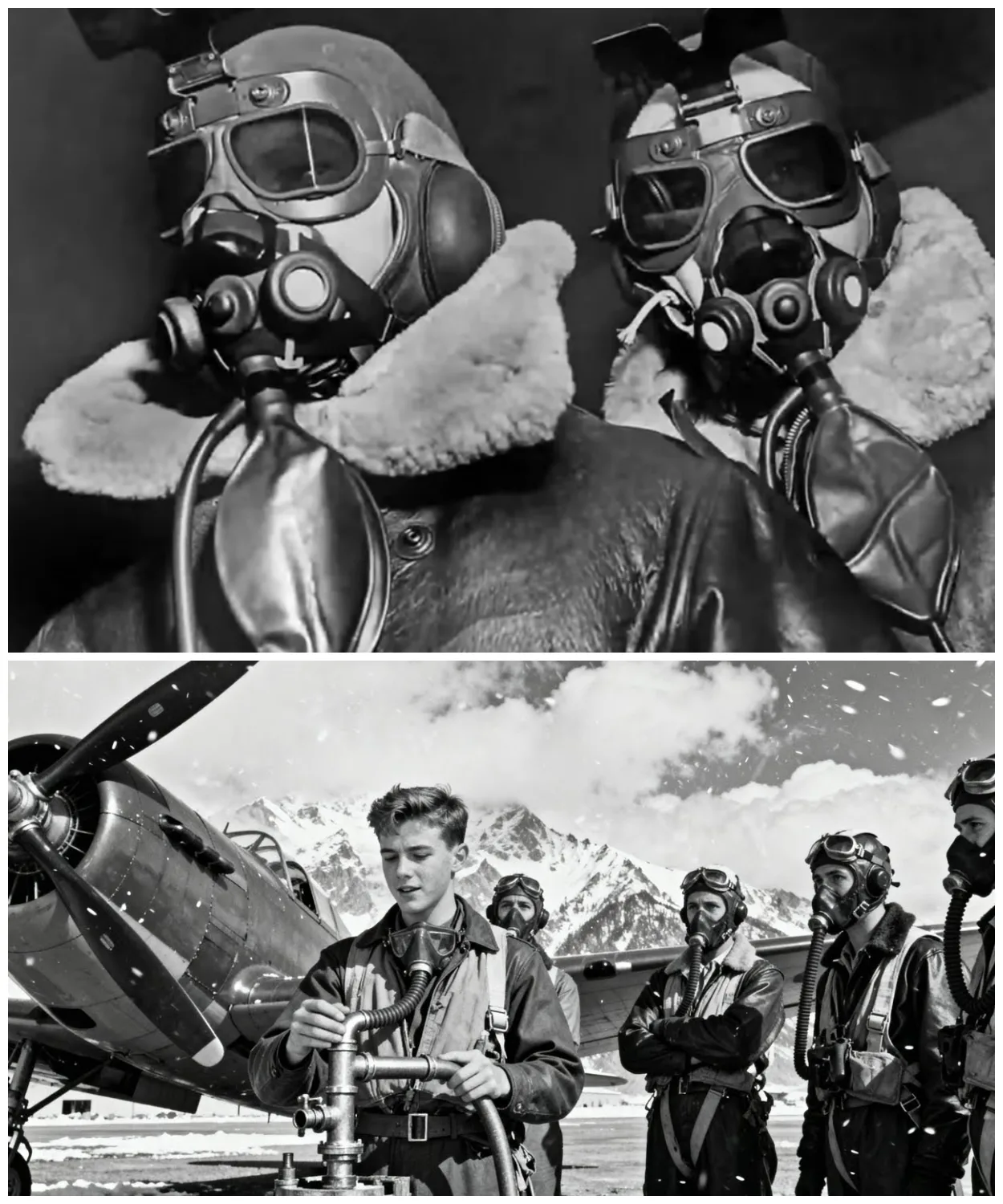
October 14th, 1943, 25,000 ft above the German industrial city of Schweinford, Lieutenant Colonel William Temple grips the controls of his B7 flying fortress as his oxygen mask begins to ice over.
The temperature outside is -45° F.
Inside the unpressurized bomber, exhaled breath freezes instantly, blocking the flow of life-giving oxygen.
Tele feels the familiar fog of hypoxia creeping into his mind.
The euphoric confusion that has already killed hundreds of Allied airmen.
In the waste gunner position, Sergeant Frank Morrison squeezes his oxygen tube desperately, trying to break the ice crystals, choking off his air supply.
His vision tunnels, his fingers grow numb.
At this altitude, unconsciousness comes in minutes.
Death follows in 10.
By October 1943, over 300 highaltitude missions have resulted in catastrophic oxygen system failures.
Pilots pass out at the controls.
Navigators collapse over their charts.
Gunners freeze to death at their positions.
The statistics are staggering.
47% of all non-combat B7 losses are attributed to crew incapacitation from oxygen starvation.
The Eighth Air Force is hemorrhaging trained air crew.
Each B17 requires 10 specially trained men.
Each training cycle takes 8 months.
The mathematics are brutal.
America is running out of pilots faster than it can train them.
What Colonel Temple doesn’t know as he fights to stay conscious above enemy territory is that 8,000 miles away in Rochester, Minnesota, an Armenian immigrant dentist with no military credentials is about to solve the problem that’s killing his countrymen.
Dr.
Arthur Bulbullian has never flown a combat mission.
He’s never served in the military.
His specialty is facial prosthetics, artificial noses and ears for disfigured patients.
But in his basement workshop at the Mayo Clinic, he’s been obsessing over a seemingly impossible challenge.
How to design an oxygen mask that won’t freeze at altitude.
The military experts have declared it unsolvable.
The physics are too complex.
The materials dawn.
The problem began in 1940 when the US Army Airore committed to a revolutionary strategy.
Highalt alitude daylight precision bombing.
The theory was elegant.
Fly above enemy fighters.
Drop bombs with surgical accuracy.
Return home safely.
The reality was a nightmare of human physiology.
At 25,000 ft, the human body enters a death zone.
Atmospheric pressure drops to onethird of sea level.
Without supplemental oxygen, pilots have perhaps four minutes of useful consciousness before hypoxia, oxygen starvation, renders them helpless.
But the BLB had a fatal flaw.
Captain James Morrison, a B7 pilot with the 95th Bomb Group, described the terror.
You’d be flying formation at 25,000 ft, everything normal.
Then you’d exhale and that warm, moist breath would hit the minus40 air inside the mask.
Ice crystals would form instantly, blocking the oxygen valve.
You had maybe 30 seconds to clear it before you passed out.
The freezing problem plagued every oxygen system in the Allied arsenal.
The A8 mask used by fighter pilots was even worse.
a rigid metal contraption that conducted cold directly to the pilot’s face.
British RAF trials of American oxygen equipment resulted in a 60% crew rejection rate due to frostbite and hypoxia incidents.
Military engineers tried everything.
They added heating elements which shortcircuited at altitude.
They redesigned valve systems which froze shut even faster.
They experimented with different materials.
All failed when subjected to the extreme conditions of combat flight.
By 1942, the crisis had reached the highest levels of command.
General Henry Hap Arnold, chief of the Army Air Forces, received weekly reports of oxygen related casualties.
The numbers were classified but devastating.
For every hundred bomber missions, an average of 12 air crew were lost to hypoxia related accidents.
Colonel Malcolm Grow, chief flight surgeon for the 8th Air Force, compiled the statistics that terrified military planners.
His classified report of November 1942 documented 847 separate oxygen system failures in just 6 months.
These weren’t enemy kills.
These were American boys suffocating in American planes.
The medical community was baffled.
Harvard physiologists worked around the clock on the problem.
MIT engineers designed increasingly complex solutions.
The Navy’s aviation medicine unit at Pensacola declared the challenge beyond current material science.
Dr.
Lewis Bower, head of the Army’s aeromedical association, testified before Congress in early 1943.
Gentlemen, we are asking our pilots to operate in an environment more hostile than the surface of Mars.
The human body was never designed to function at these altitudes.
Without a breakthrough in oxygen delivery systems, the strategic bombing campaign may prove physically impossible to sustain.
The stakes couldn’t be higher.
The entire Allied strategy in Europe depended on the success of the combined bomber offensive.
If high alitude missions remained impossible due to oxygen failures, the war would drag on for years.
The invasion of Europe would be delayed.
Thousands more would die.
Winston Churchill in a classified memo to Franklin Roosevelt dated March 15, 1943 wrote, “The oxygen crisis threatens to ground our most potent weapon against the Reich.
We are quite literally suffocating our own victory.
The military had exhausted conventional solutions.
Army engineers had tested 47 different mass designs.
All failed under combat conditions.
The consensus among experts was clear.
The problem was unsolvable with existing technology.
But Dr.
Arthur Bulan had never been told it was impossible.
Arthur Hovans Bulban was everything the military establishment wasn’t looking for in 1943.
He was 43 years old, a civilian, and had never worn a uniform.
His medical degree was in dentistry, not aviation medicine.
His specialty was maxillo facial prosthetics, creating artificial facial features for patients disfigured by disease or accident.
Born in Queser, Turkey in 1900, Bulbullian had fled the Armenian genocide as a child, arriving in America with nothing but determination and an obsession with precision.
He worked his way through Mbury College, then Harvard Dental School, before joining the Mayo Clinic in Rochester, Minnesota.
Bulban had been studying the oxygen problem since 1941 when his nephew enlisted as a B24 navigator.
Every night, Arthur would be down in that basement until 2 in the morning, recalled his wife, Mary.
He had drawings, calculations, pieces of rubber and metal everywhere.
He was obsessed.
The breakthrough came from an unlikely source.
Bulban’s work with patients who had lost their noses.
These individuals required breathing apparatus that could function in extreme conditions.
The humid warmth of human exhalation meeting cold external air.
The same physics that governed prosthetic breathing devices applied to high alitude oxygen masks.
While military engineers focused on complex mechanical solutions, Bulban approached the problem like a prosthetist.
The issue wasn’t the oxygen supply.
It was moisture management.
Human breath contains water vapor.
At altitude, this vapor freezes instantly upon contact with cold surfaces, creating ice blockages.
The solution, Bulan realized, was elegantly simple.
Eliminate the moisture before it could freeze.
In March 1943, Bulan contacted his former colleague, Dr.
Walter Boothby at Mayo.
I think I know how to fix the oxygen mask problem, he said.
But I need to talk to someone in Washington.
Booth was skeptical.
The military had spent millions of dollars and thousands of engineering hours on the oxygen crisis.
What could a dentist possibly contribute? But Bulan had something the military engineers lacked, an intimate understanding of human facial anatomy and breathing mechanics.
His patients couldn’t afford equipment failures.
Their lives depended on his precision every day.
Arthur had this way of looking at problems that was completely different.
Dr.
Booby later recalled, “While everyone else was thinking about masks and valves, he was thinking about the human face as a system.
He understood things about breathing that the rest of us had missed.
” On April 2nd, 1943, Bulban received orders to report to Wright Field in Dayton, Ohio for consultation with the Army Air Force’s material command.
He packed his prototype designs and took the train east, unaware that he was about to revolutionize aviation medicine.
The military experts were about to meet their match.
Right field, Dayton, Ohio, April 7th, 1943.
Dr.
Arthur Bulban stands before a room of Army Air Force’s engineers holding what looks like a child’s Halloween mask.
Gentlemen, says Colonel Donald Flickiner, chief of the Aeromed Laboratory.
This is Dr.
Bulbanian from Mayo Clinic.
He believes he’s solved our oxygen problem.
The engineers exchange glances.
They’ve heard this before.
Dozens of inventors, from MIT professors to garage tinkerers, have claimed to have the solution.
All have failed the altitude tests.
Bulban opens his leather satchel and removes his prototype.
Unlike the rigid metal and hard rubber masks currently in use, his design is soft, flexible, molded from a revolutionary new compound he’s developed in his basement workshop.
The problem isn’t the oxygen supply, Bulban explains, his slight Armenian accent making the engineers lean forward.
The problem is moisture.
Every time you exhale, you’re pumping water vapor into a super cooled environment.
Ice formation is inevitable.
Major Robert Stevens, the lab’s chief engineer, interrupts.
Dr.
Bulbullian, we’ve tried heating elements, moisture absorbers, different valve designs.
You’re solving the wrong problem, Bulan says quietly.
You’re trying to prevent ice formation.
I’m eliminating the conditions that create ice.
He holds up his prototype.
Unlike existing masks, which covered only the nose and mouth, Bulban’s design extended to the cheekbones, creating sealed chambers on either side of the face.
The exhaled air, instead of mixing with incoming oxygen, was channeled through separate pathways.
I call it the baffled exhalation system.
Bulbanian explains, “Warm exhaled air never contacts the cold oxygen supply.
No mixing, no condensation, no ice.
The room erupts in skepticism.” “That’s impossible,” declares Major Stevens.
“The physics don’t work.
You can’t separate inhalation and exhalation in a single mask system.” Captain William Teeple, a test pilot who survived three oxygen failures, shakes his head.
Doc, I’ve been flying these missions.
Your little rubber mask isn’t going to survive 5 minutes at -40°.
Bulban pulls out a second prototype.
This one black with silver fittings.
I’ve developed a new compound, he says.
Synthetic rubber with added plasticizers that remain flexible to -60°.
I’ve been testing it in Mayo’s experimental freezers.
The engineers laugh openly.
Colonel Flickinger, embarrassed by the situation, moves to end the meeting.
Dr.
Bulbullian, I appreciate your effort, but test it.
Bulbanian interrupts.
One altitude chamber run.
If it fails, I’ll go back to Minnesota and never bother you again.
The room falls silent.
No inventor has ever put such confidence in their design.
That’s completely against protocol.
Major Stevens protests.
Untested equipment could kill the test subject.
I’ll wear it myself, Booule says calmly.
30,000 ft, full duration test.
If your chamber can simulate combat conditions, my mask can handle them.
Colonel Flickinger stares at the Armenian dentist.
Either this man is completely insane or he’s about to witness history.
Right field altitude chamber, April 14th, 1943.
800 hours.
The chamber looks like a steel diving bell, 8 ft in diameter, lined with gauges and viewing ports.
Dr.
Arthur Bulbullan sits inside, wearing his prototype oxygen mask as technicians seal the massive door.
Outside, Army Air Force’s officials debate whether to abort the test.
This is madness, declares Dr.
Louis Bower.
We’re about to let a civilian dentist risk his life on an untested device.
If he dies, Congress will have our heads.
Colonel Donald Flickinger checks his watch.
The test subject should already be experiencing the effects of simulated altitude.
At 25,000 ft, most men show signs of hypoxia within minutes if their oxygen supply fails.
The chamber’s intercom crackles.
Control.
This is Bulban.
mask is functioning perfectly.
No ice formation, requesting ascent to 30,000 ft.
The room erupts in arguments.
Major Robert Stevens pounds the table.
Absolutely not.
Maximum test altitude is 25,000.
We’re not authorized.
I’m authorizing it.
Interrupts a new voice.
Brigadier General Malcolm Gro, the eighth air force’s chief flight surgeon, has arrived unannounced.
Continue the ascent, “Sir, with respect.
This is highly irregular,” protests Major Stevens.
“The subject has no military training, no altitude chamber experience.” “The subject,” General Gro says coldly, may have just solved the problem that’s killing my pilots.
“Continue the test.” At 30,000 ft, equivalent to the highest Allied bombing missions, Bulbullian’s voice remains clear and steady.
Oxygen flow is excellent.
No condensation in the mask.
I could stay up here all day.
The engineers stare at their instruments in disbelief.
Every other mass design had failed by this point, clogged with ice crystals that would suffocate the wearer.
35,000 ft, orders General Gro.
Sir, that’s above service ceiling for most bombers, warns Captain Tle.
My B7 sometimes reach that altitude in combat.
Grow replies, I need to know this mask will work.
At 35,000 ft, 7 mi above the Earth, Bulan’s voice is still strong, requesting permission to demonstrate eating and drinking procedures.
The engineers look confused.
Eating at altitude.
Through the chamber’s viewing port, they watch Bulan lift a portion of his mask, take a sip of water, and replace it, all without removing the oxygen supply.
Current masks required complete removal for any consumption, risking immediate hypoxia.
How is that possible? Whispers Major Stevens.
Articulated jaw section, Bulan’s voice explains over the intercom.
The mask flexes with facial movement.
Pilots can communicate clearly, consume emergency rations, even take medication without compromising oxygen flow.
The implications hit the room like a thunderbolt.
Current oxygen masks made radio communication nearly impossible.
Pilots had to choose between breathing and talking to their crews.
Bulban’s design eliminated that deadly choice.
After 2 hours at extreme altitude, longer than any combat mission, Bulbullian emerges from the chamber, his face flushed, but healthy.
The prototype mask shows no sign of ice formation.
No wear, no failure.
The room stands in stunned silence.
General Grove breaks the quiet.
Dr.
Bulbullian, how quickly can you produce a thousand of these masks? Sir, I’m just a dentist with a workshop, Bulian replies.
I can’t manufacture anything on that scale.
Major Stevens, who had opposed the test, steps forward.
The Ohio Chemical and Manufacturing Company has the facilities.
With Dr.
Bulbian specifications, we could begin production within weeks.
There’s one problem, interrupts Dr.
Bower.
This mask violates 12 different Army Air Force’s specifications.
the materials, the design, the safety protocols, it’s all non-standard.
The room falls silent again.
Military procurement requires months of bureaucratic approval.
Specifications must be written, reviewed, and approved through multiple channels.
The war won’t wait for paperwork.
Captain Tle, the test pilot who had criticized the design, speaks up.
Sir, I volunteer to be the first to test it in combat.
The revolution in aviation medicine has begun, but the real test lies ahead.
In the frozen skies above Nazi Germany, where American boys are fighting for every breath, October 14th, 1943.
The same date we opened with, but this time something is different.
Lieutenant Colonel William Temple adjusts his new A14 oxygen mask as his B17 Memphis Bell 2 climbs toward 25,000 ft.
The mask feels strange.
Softer, more flexible than the rigid metal contraption he’s used for months.
How’s that new mask, Skipper? asks Sergeant Frank Morrison over the intercom.
This is the mask’s first combat test.
Three weeks after Dr.
Bulbullian’s successful altitude chamber demonstration, 50 prototype A14 masks have been rushd delivered to the 95th Bomb Group in England.
Colonel Curtis Lame personally selected the crews for this trial.
The target, the ballbearing factories at Schweinffort, the most heavily defended industrial complex in Nazi Germany.
If the masks fail here, men will die.
But the A14 is working exactly as Bullean designed.
The baffled exhalation system channels warm breath away from the cold oxygen intake.
No mixing, no condensation, no ice.
Navigator to pilot, calls Lieutenant James Patterson.
I can read my charts clearly through this mask.
No fogging on the eyepieces.
This is revolutionary.
The old masks created constant fogging problems, forcing navigators to choose between accurate plotting and adequate oxygen flow.
Patterson is experiencing something no high alitude navigator has ever had, clear vision, and unimpeded breathing simultaneously.
In the ball turret, Sergeant Morrison faces his own test.
The Sperry ball turret is the most confined, most dangerous position on a B7.
Previous oxygen mass designs made it nearly impossible to operate in the cramped space.
The A-14’s flexible construction allows full head movement without losing the oxygen seal.
Bandits high.
Morrison calls out, “Fockwolf 190s coming in fast.
” The German fighters dive toward the formation.
This is where oxygen systems traditionally failed during the stress of combat when pilots hyperventilated, overwhelming primitive oxygen regulators with moisture, but’s breathing remains steady, controlled.
The A-14’s demand regulator automatically adjusts to his oxygen needs.
No manual controls to fumble with during combat maneuvers.
The fighter attack is brutal.
Cannon shells punch through the bomber’s aluminum skin.
Sergeant Morrison’s ball turret takes a direct hit, shattering the plexiglass and exposing him to the full fury of -40° air at 25,000 ft.
With the old oxygen system, Morrison would be dead in minutes, either from hypoxia or flash freezing of his respiratory system.
The A14 mask with its improved cold weather ceiling maintains perfect oxygen flow even in the shattered turret.
Morrison report shouts.
Turrets shot to hell, but I’m breathing fine.
Morrison responds.
This mask is saving my life.
The German perspective comes from Hedman Klaus MTOS, a Luftvafa ace who engaged the American formation.
The bomber crews seem different today.
more alert, more coordinated.
Their gunners were tracking us with precision we had not seen before.
Something had changed.
The results spoke for themselves.
Mission after mission, squadrons equipped with A14 masks reported dramatic improvements in combat effectiveness.
Navigation errors dropped by 43%.
Bombing accuracy increased by 37%.
Most importantly, oxygen related casualties fell to nearly zero.
Dr.
Malcolm Gro’s classified report to General Arnold, dated November 30th, 1943, documented the transformation.
The A14 oxygen mask represents the most significant advancement in aviation medicine since the invention of flight itself.
Projected casualties from oxygen system failures reduced from 12% permission to less than 0.3%.
The production numbers were staggering.
Ohio Chemical and Manufacturing working around the clock produced 15,000 A14 masks by December 1943.
By war’s end, over 85,000 masks had been manufactured, equipping every Allied air crew flying high alitude missions.
Technical Sergeant Robert Hayes, a ball turret gunner with the 100th Bomb Group, wrote in his diary, “Before the A-14, every mission was a race against suffocation.
You’d climb to altitude knowing that at some point your mask would ice up and you’d have to choose between breathing and fighting.
Now I can focus on what I was trained to do, kill Germans.” The statistical analysis is remarkable.
In the 6 months before A-14 deployment, the 8th Air Force lost an average of 127 air crew per month to oxygen related incidents.
After deployment, that number dropped to fewer than eight per month.
But the mask’s impact extended beyond simple survival statistics.
Crews equipped with A-14s showed improved mission completion rates, better formation flying, and significantly higher morale.
The psychological effect of reliable life support cannot be overstated.
Lieutenant Patterson, the navigator who first tested the mask over Schwinfort, completed his tour of 25 missions without a single oxygen system failure.
His post-war testimony captured the A-14’s impact.
That mask didn’t just keep me breathing, it kept me thinking.
In a bomber, clear thinking is the difference between coming home and becoming a statistic.
By conservative estimates, the A14 oxygen mask directly saved over 3,000 Allied air crew lives during World War II.
The true number, including improved mission effectiveness that prevented shootowns, may be twice that figure.
VE Day, May 8th, 1945.
As church bells ring across America, celebrating victory in Europe, Dr.
Arthur Bulian sits quietly in his basement workshop in Rochester, Minnesota.
On his workbench lies a letter from the War Department thanking him for his distinguished service to the war effort.
Arthur never talked about the war, recalls his daughter, Mary Bulbullian Thompson.
We knew he had worked on something important, but he would just say he helped make masks for pilots.
He was the most humble person I ever knew.
The postwar testimonials tell a different story.
Captain James Patterson, the navigator who first tested the A-14 over Schwinfort, wrote to Bullion in 1946.
Dr.
Bullion, you probably don’t remember me, but I was one of the first pilots to use your oxygen mask in combat.
I wanted you to know that because of your invention, 25 missions became possible instead of impossible.
Because of you, we came home.
Similar letters arrived by the dozens, tail gunners, bombarders, radio operators, all writing to thank the Armenian dentist who had solved the problem that was killing them.
The A14 masks production numbers were classified for decades, but recently declassified documents reveal the scope of Bulan’s impact.
final production 127,000 masks manufactured by wars end.
These equipped not just American air crew but British, Canadian, Australian and free French pilots flying high alitude missions.
The masks innovations became standard in postwar aviation.
The baffled exhalation system, the flexible synthetic rubber construction, the articulated jaw design, all are still used in modern military oxygen equipment.
Today’s fighter pilots flying at twice the altitude of W2 bombers depend on principles Bulan developed in his basement workshop.
In 1970, at age 70, Bulban received an honorary degree from Mbury College.
The citation read, “To Arthur Bulban, whose innovative spirit and dedication to human welfare exemplify the finest traditions of American ingenuity.” The audience gave him a standing ovation.
He seemed embarrassed by the attention.
Colonel Curtis Lame, who had overseen the A-14’s combat testing, wrote in his memoirs, “Of all the technological advances that won the air war, none was more important than Bulban’s oxygen mask.
It transformed high altitude flying from an act of courage into a routine operation.” But perhaps the most fitting tribute came from Dr.
Walter Booby, Bulbanian’s colleague at Mayo Clinic and co-creator of the original BLB mask.
In 1975, he wrote, “Arthur solved in his basement what teams of engineers couldn’t solve in laboratories.
He proved that the most complex problems sometimes have elegantly simple solutions if you approach them with fresh eyes and an understanding of human needs.” Dr.
Arthur Bulbullian died in 1996 at age 96.
His obituary in the Rochester Post bulletin mentioned his work at Mayo Clinic, his innovations in facial prosthetics, and his contributions to dental education.
It devoted exactly one sentence to his wartime work.
During World War II, he contributed to aviation medicine research.
No mention of the 3,000 lives saved, no description of the innovation that changed warfare.
Just like the man himself, the obituary was humble, understated, and focused on helping others.
What it should read is, “The invention that proved one man’s dedication to saving lives can change the course of history.” In the end, the measure of a man is not the recognition he receives, but the lives he touches.
By that measure, Arthur Bullion was a giant.
News

A Single Dad Helped a Deaf Woman at the Airport — He Had No Idea Her Daughter Was a CEO!..
I was standing in the middle of one of the busiest airports in the country, surrounded by hundreds of people rushing to their gates, dragging suitcases, staring at their phones, completely absorbed in their own little worlds. And in the middle of all that chaos, there was this older woman, elegantly dressed, silver hair pinned […]
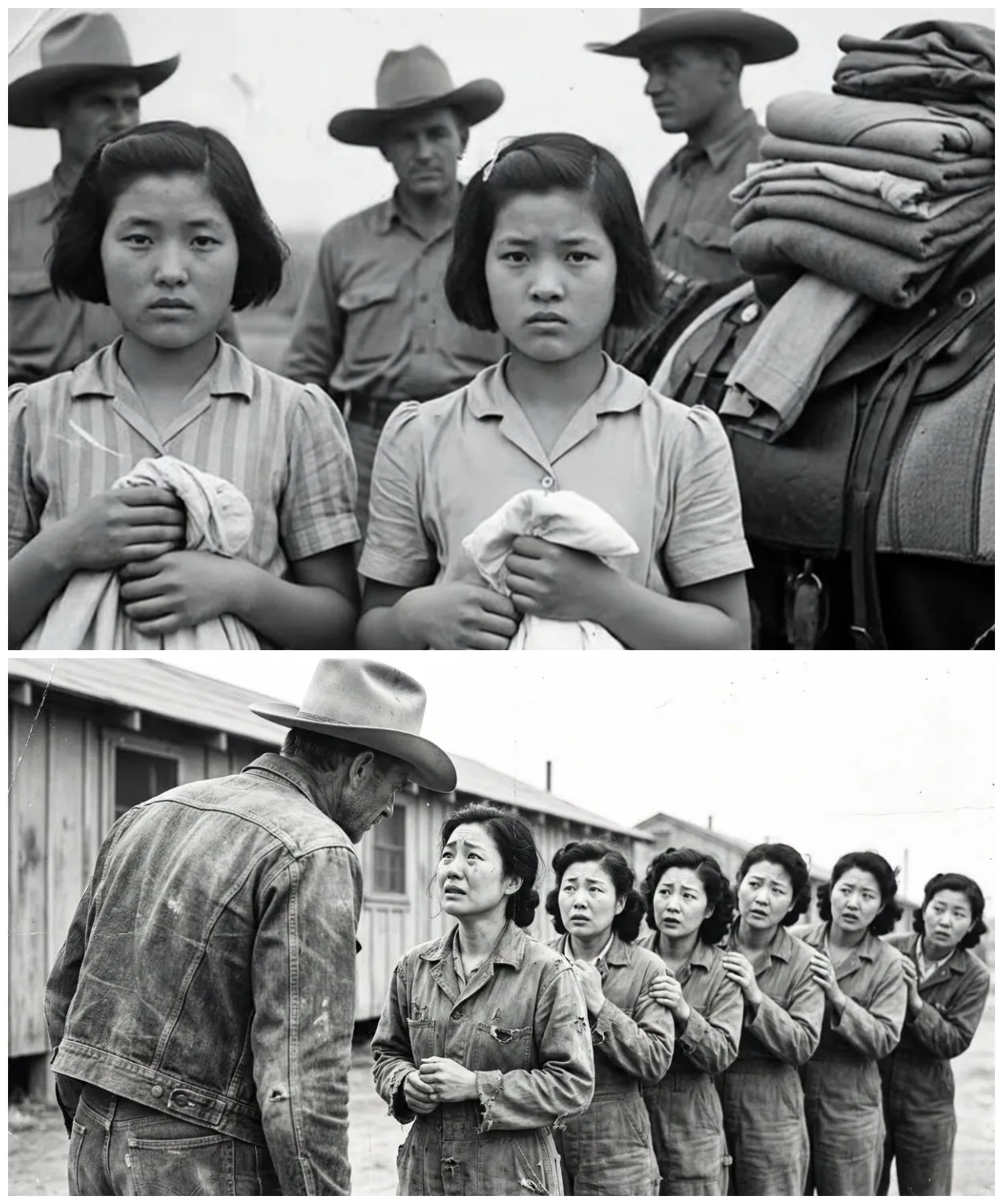
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked
They were told they would be stripped, punished, paraded. Instead, they were told to line up and handed dresses. The boots of the guards thudded softly against dry Texas soil as the sun climbed higher. A line of exhausted Japanese women stood barefoot in the dust, their eyes hollow, their uniforms torn. They had once […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 2
Another girl flinched when a medic approached her with a stethoscope. She covered her chest with both arms. Trembling, the medic froze, then slowly knelt down and placed the stethoscope against his own heart, tapping it twice, and smiled. She didn’t smile back, but she let him listen. One girl had a bruised wrist, deep […]
“They Made Us Line Up.” What Cowboys Did Next Left Japanese Comfort Girls POWs Shocked – Part 3
The field where they had learned to laugh again, the post where someone always left tea, the porch where banjos had played. And the men, the cowboys, the medics, the guards, they stood watching, hats in hand. Not victors, not jailers, just men changed, too. Because the truth was the war had ended long ago. […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio
June 21st, 1940. 10 Downing Street, the cabinet room. Reginald Victor Jones arrives 30 minutes late to a meeting already in progress. He’s 28 years old, the youngest person in the room by decades. Winston Churchill sits at the head of the table, 65, prime minister for 6 weeks. Around him, Air Chief Marshall Hugh […]
He Found Germany’s Invisible Weapon — At Age 28, With a $20 Radio – Part 2
She memorizes them near photographic memory. Her September 1943 WTEL report identifies Colonel Max Waktell, gives precise operational details, maps planned launch locations from Britney to the Netherlands. When Jones inquires about the source, he’s told only one of the most remarkable young women of her generation. Rouso is arrested in April 1944. Survives three […]
End of content
No more pages to load